



Home / Training / Manuals / Atlas of breast cancer early detection / Learning
.png)
Click on the pictures to magnify and display the legends

Click on this icon to display a case study
Atlas of breast cancer early detection
Filter by language: English / РусскийClinical breast examination (CBE) Common abnormalities |
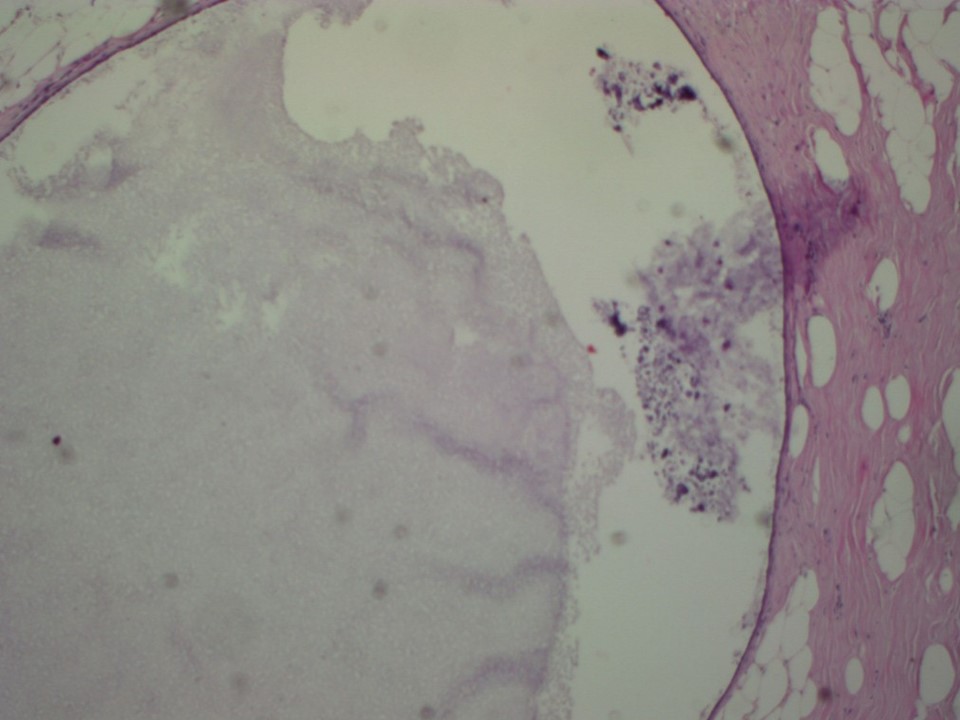
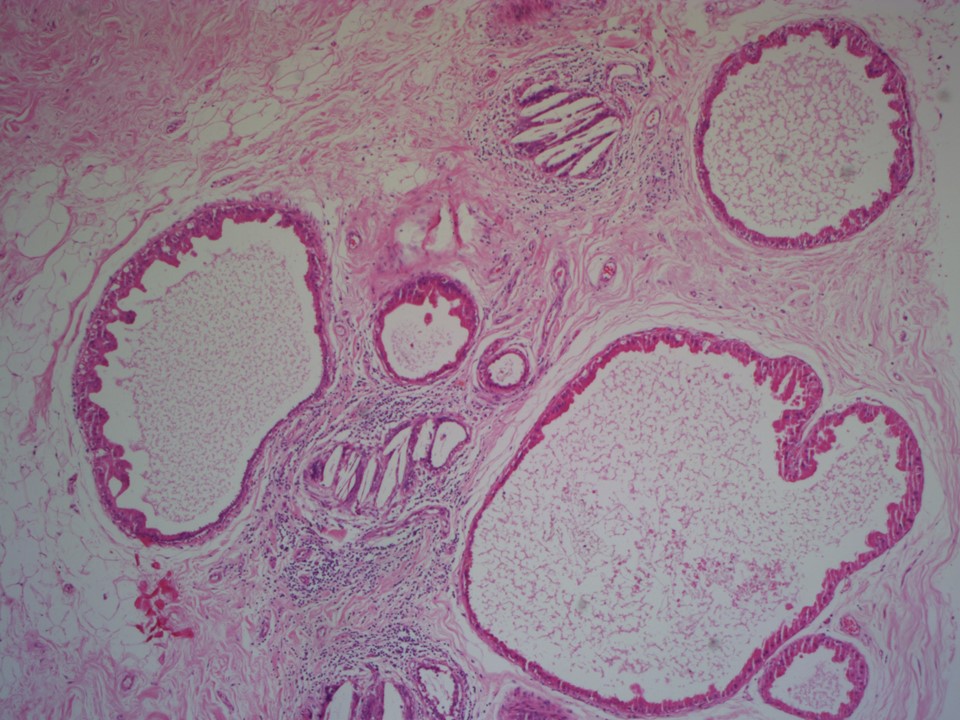
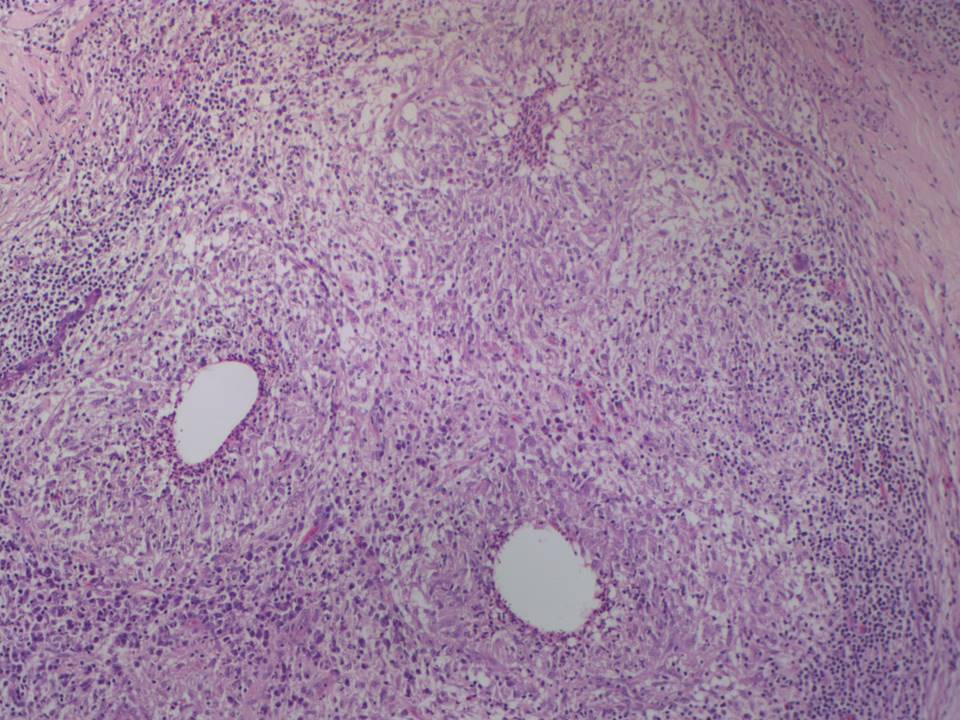
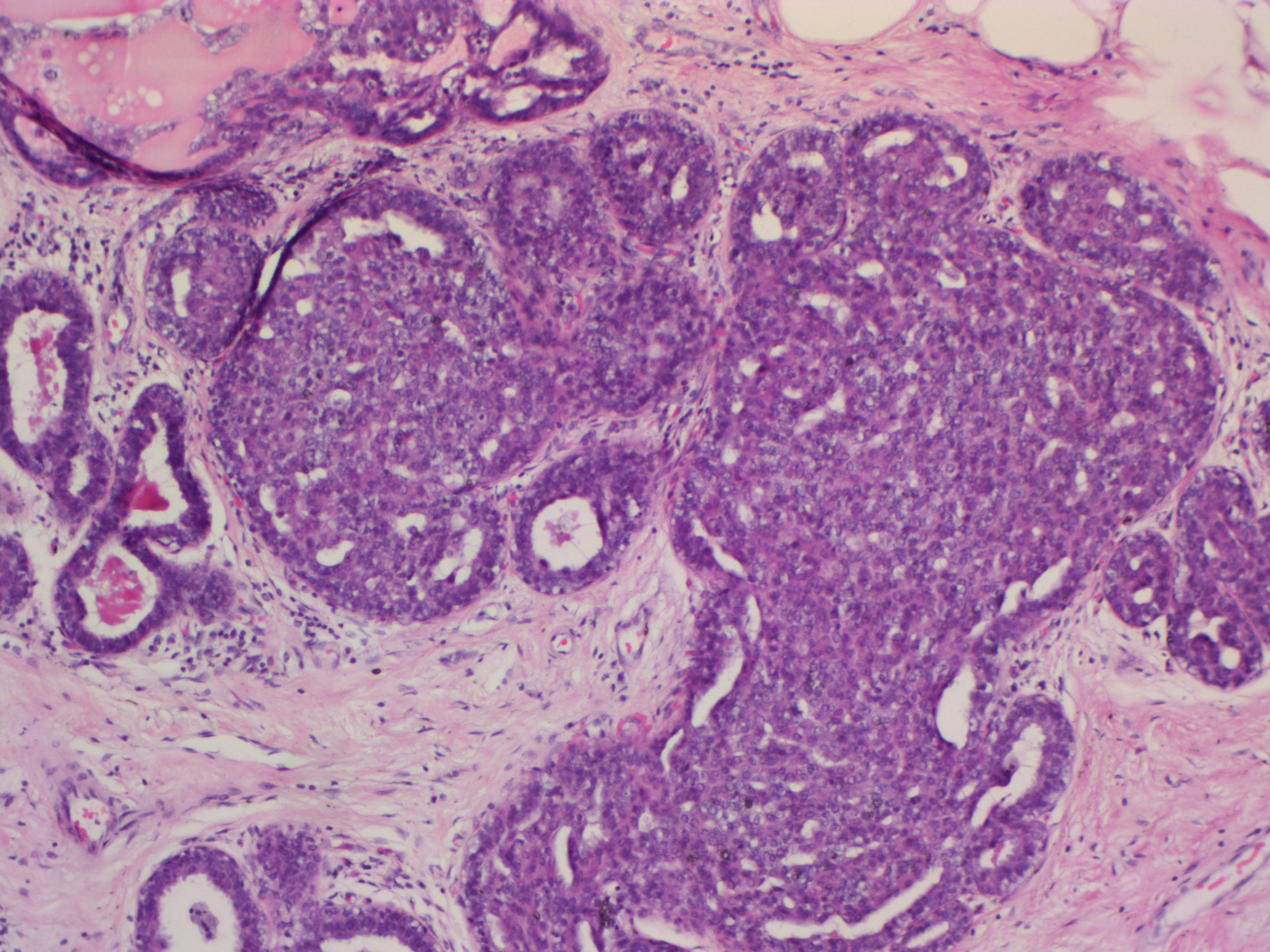
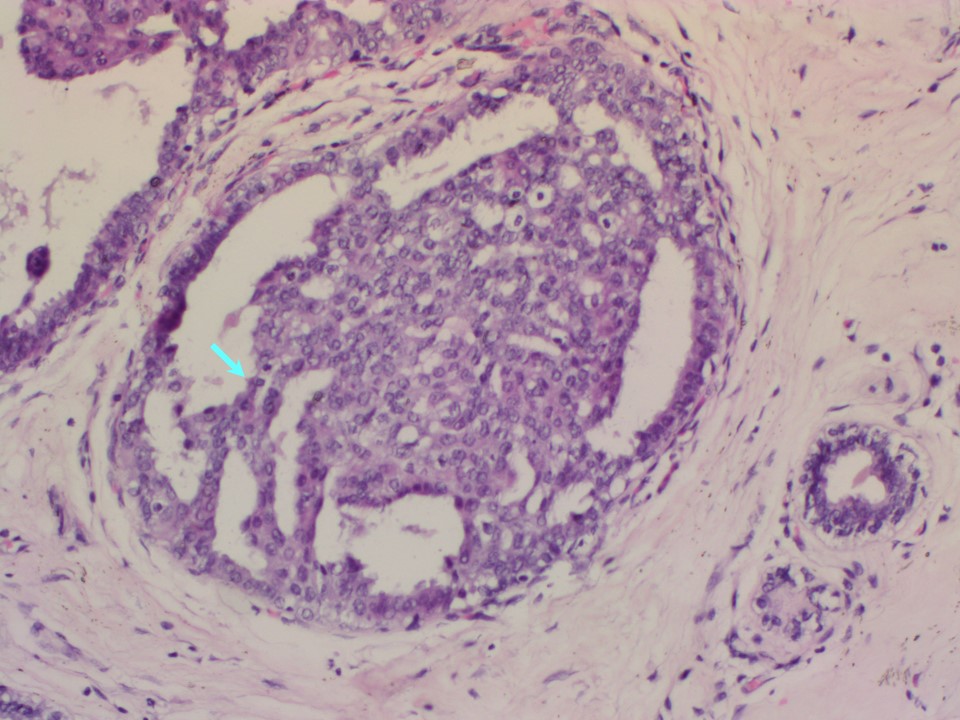
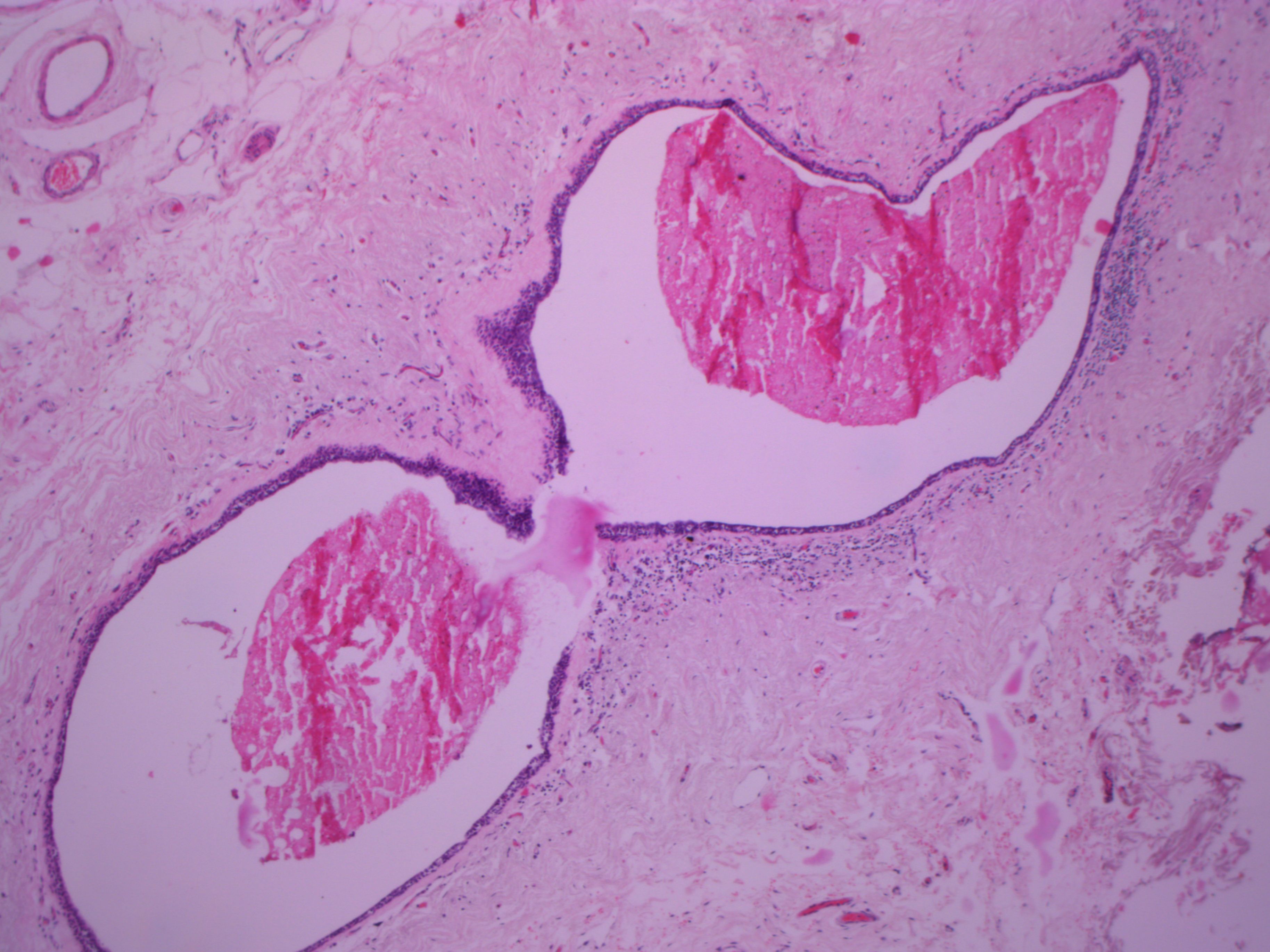
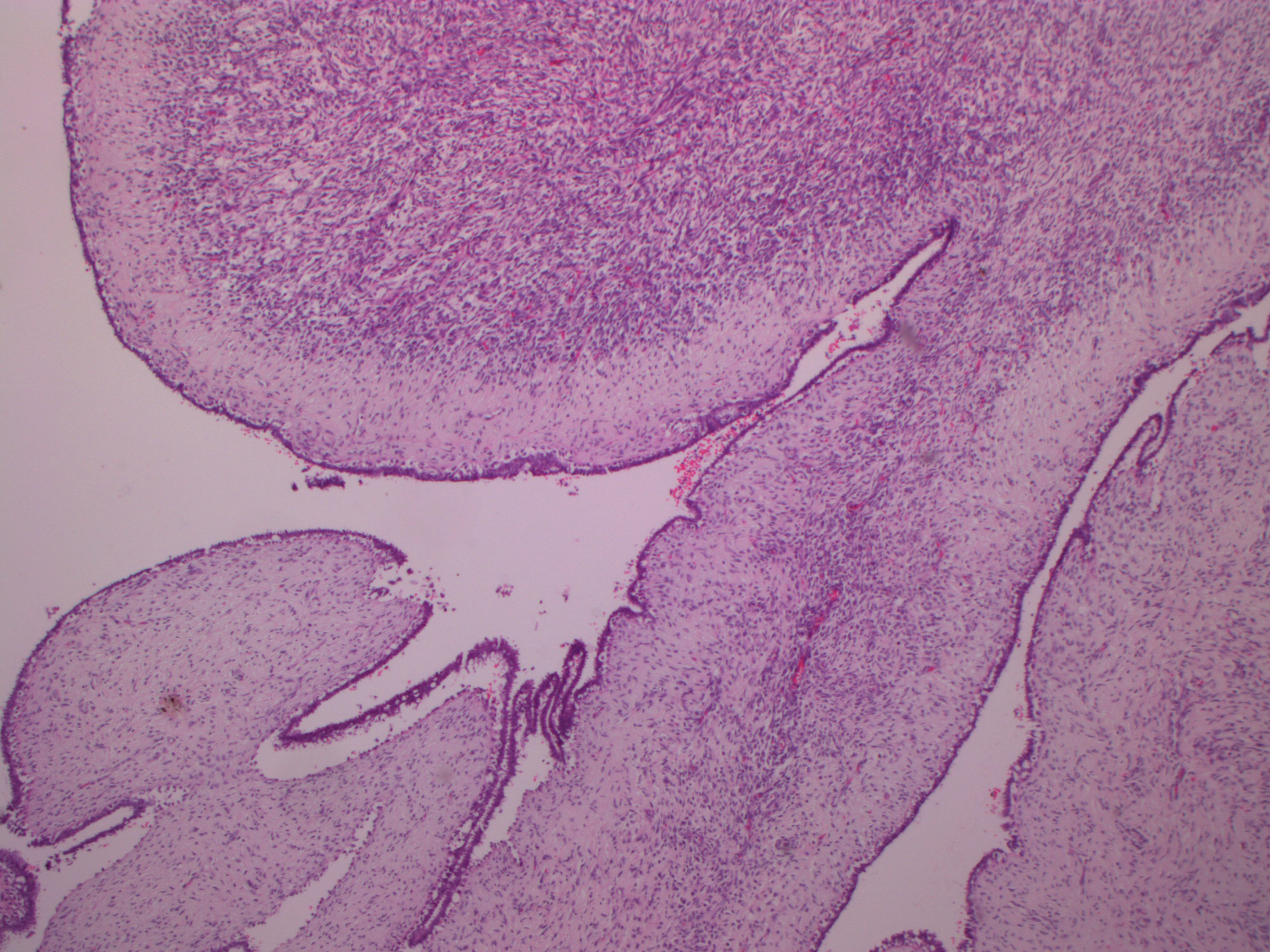
The primary aim of CBE is to detect malignant lesions of the breast. However, CBE can detect some of benign conditions for which further management may be required. Benign conditions often encountered during the breast examination include fibroadenoma, cysts, fibrocystic breast, inflammatory conditions of the breasts, and intraductal proliferative lesions. Fibroadenoma Fibroadenoma is a common benign tumour of the breast often seen in young women. A fibroadenoma usually has a soft to firm texture, is smooth to the touch, and moves easily under the skin. For this reason it is sometimes called a breast mouse. Fibroadenomas are usually painless and sometimes there is more than one in the breast. They often develop during puberty and so are mostly found in young women, although they can occur in women of any age. Most fibroadenomas are about 13 cm across. Fibroadenomas larger than 5 cm across are called giant fibroadenomas. Diagnosis can be confirmed by ultrasound alone (in women younger than 30 years) or ultrasound and mammography followed by FNAC. Fibroadenomas may be excised or left alone, especially in young women. Breast cysts Cysts are fluid-filled dilated ducts or lobules that develop in the breast tissue. They develop naturally as the breast ages. Although breast cysts may be detected at any age, they are most common in women older than 35 years who have not yet reached the menopause. Cysts may feel soft during CBE if they are near the surface of the breast, or may be felt as hard lumps if they are deeper in the breast tissue. For some women the cysts can be uncomfortable and even painful, especially before menstruation when the cysts may become larger and feel sore and tender. The cysts are often multiple and may be present in both breasts. When they are detected as lumps, further investigations are warranted. When confirmed as cysts on triple assessment, they can be left alone with reassurance to the woman. Fibrocystic breast Fibrocystic changes of the breast are common findings during CBE and are more commonly seen in premenopausal women. The breasts may feel lumpy or nodular with fine nodularity. No definite lump is felt. Signs and symptoms of fibrocystic breasts may include pain and tenderness to touch. Similar findings are often seen in both breasts. These changes in the texture and lumpiness of the breasts sometimes change with phases of menstruation. These changes need reassurance only. The woman is encouraged to self-examine her breasts every day of the menstrual cycle initially, to become familiar with these cyclical changes. Inflammatory conditions of the breasts Mastitis or acute inflammation of the breast tissue occurs mainly during the lactational period. The cause of lactational mastitis is infection of a blocked milk duct. If a breast does not completely empty at feedings, one of the milk ducts can become clogged. The blockage causes milk to stagnate, leading to breast infection. Infection may lead to collection of pus, which is known as a breast abscess. On examination, the breast has a painful and tender lump with a soft feel. The breasts may be enlarged. The surface of the lump is often red in colour and is warm to touch. Chronic granulomatous mastitis is a condition that develops when inflammation and a lump have been present for a longer period and may be associated with pain. The woman may present at any age with a lump, which is sometimes hard. This condition is very difficult to differentiate from cancer and needs biopsy for confirmation. Intraductal proliferative lesions
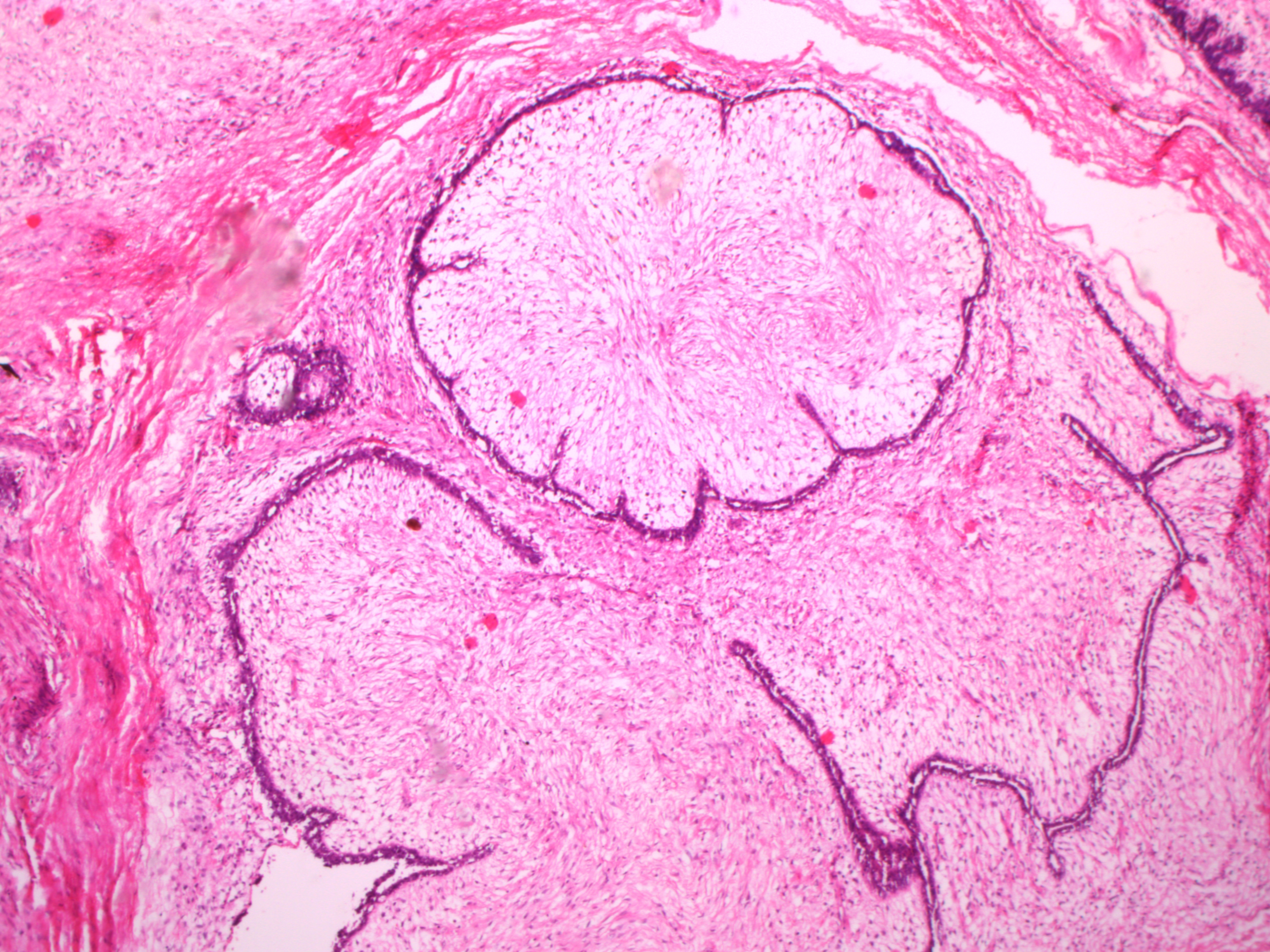
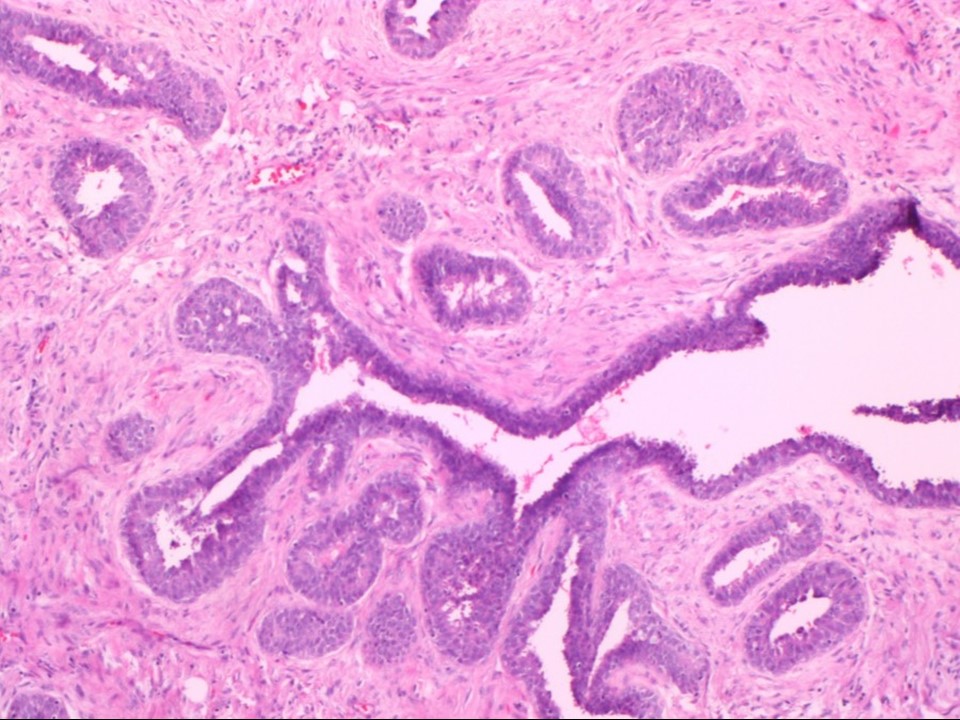
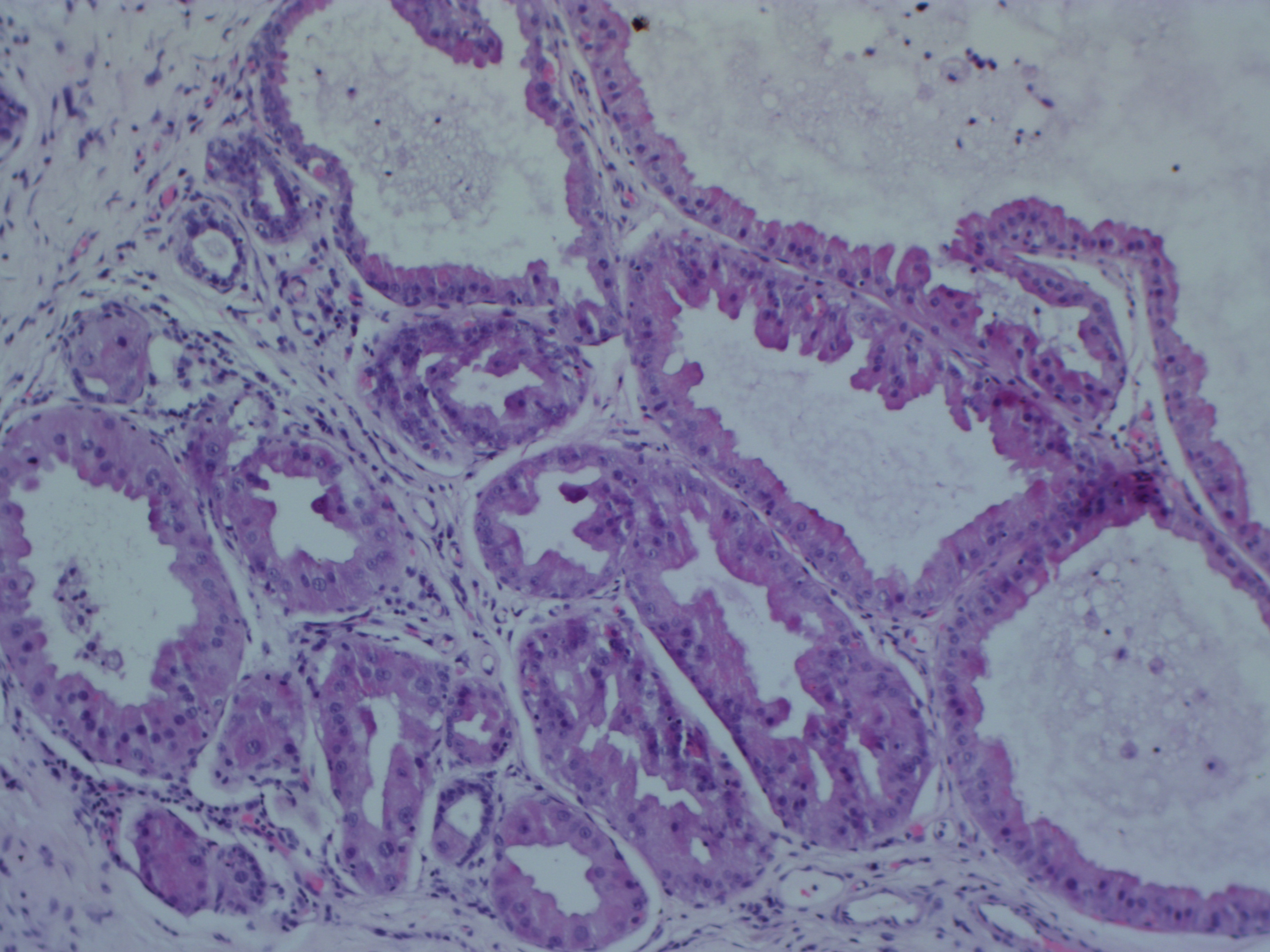
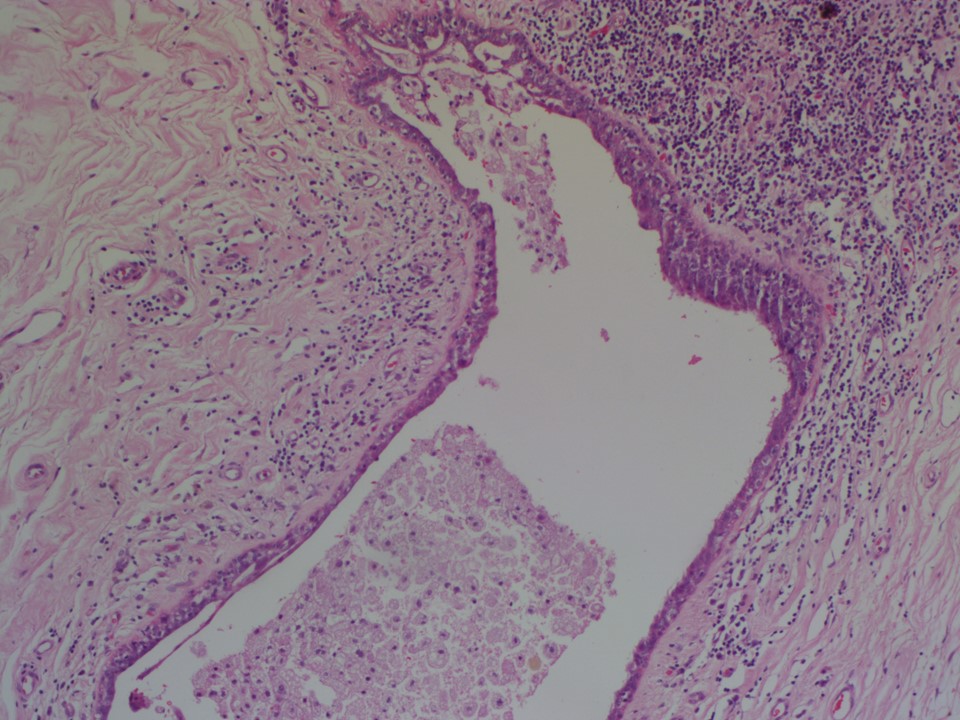
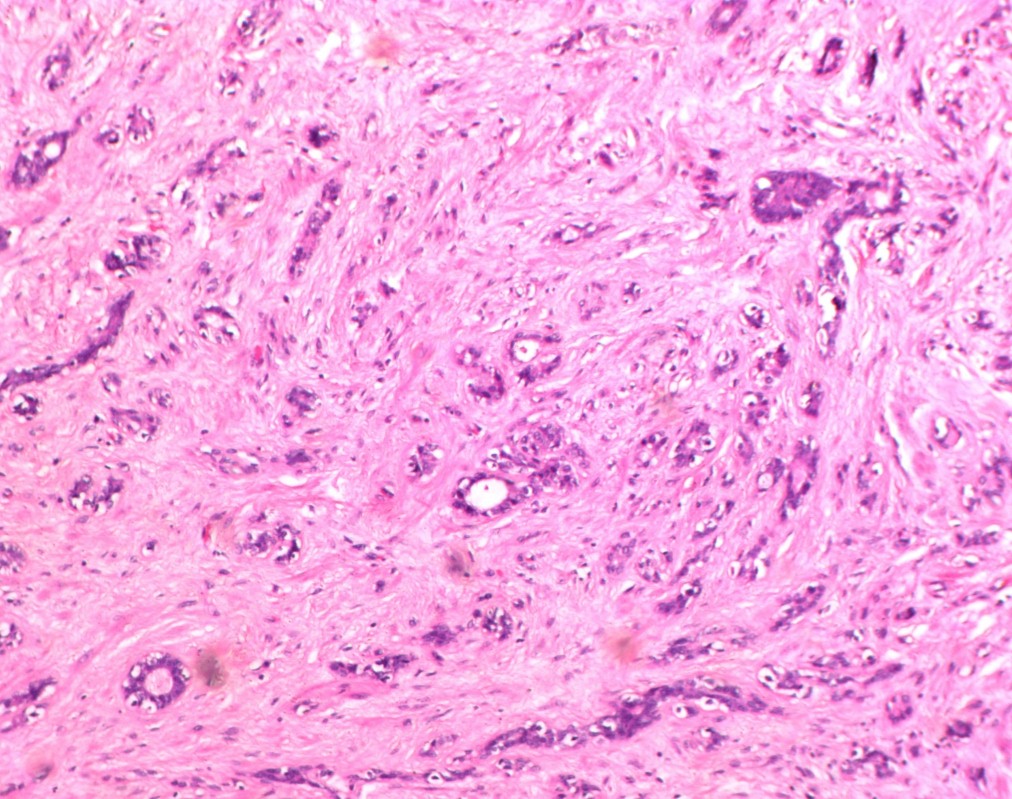
Other common benign abnormalities These entities are fat necrosis , duct ectasia , microcysts , apocrine changes , fibroadenoma , phyllodes tumour , intraductal papilloma , sclerosing adenosis
, and radial scar/complex sclerosing lesion. The morphological features of each are shown in the case studies section.
Malignant lump Breast cancer usually presents as a painless lump in the breast. It can have other manifestations such as nipple retraction, nipple excoriation, nipple discharge, skin changes, or a change in the size or contour of the breast. The malignant lump usually feels hard and has an irregular surface contour. The lump has little mobility within the breast tissue. Mobility over the pectoralis major muscle may be restricted. In advanced stages, it may be fixed to the skin or cause skin changes and ulceration. Occasionally, inflammatory carcinoma or carcinomas at advanced stage may present with features resembling inflammation, such as an enlarged tender breast or thickened red skin. |
.jpg)
.jpg)

Click on the pictures to magnify and display the legends
Click on this icon to display a case study
25 avenue Tony Garnier CS 90627 69366, LYON CEDEX 07 France - Tel: +33 (0)4 72 73 84 85
© IARC 2026 - Terms of use - Privacy Policy.
© IARC 2026 - Terms of use - Privacy Policy.