



Home / Training / Manuals / Atlas of breast cancer early detection / Learning
.png)
Click on the pictures to magnify and display the legends

Click on this icon to display a case study
Atlas of breast cancer early detection
Filter by language: English / РусскийBreast pathology Introduction |
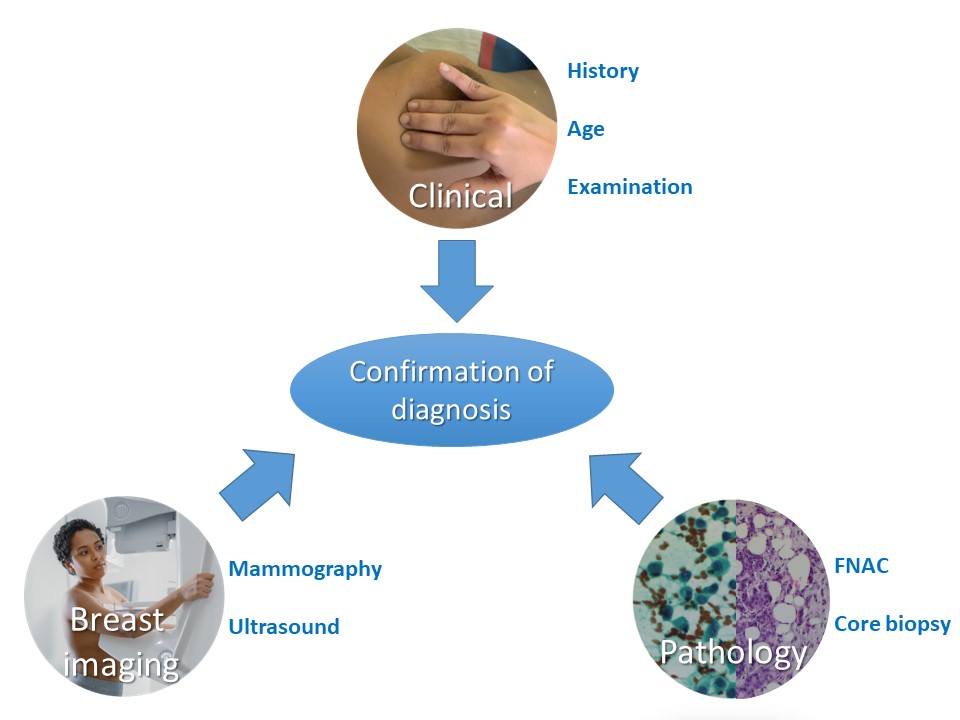
An accurate pathological diagnosis is crucial for determining the course of breast cancer treatment and estimating the prognosis with reasonable accuracy. Pathology is one of the key elements of triple assessment for the evaluation of a woman with an abnormal screening test or a woman with clinical and/or radiological suspicion of breast lesion. Ensuring quality at every step of breast pathology from sample collection to final reporting is absolutely essential to provide standardized evidence-based care to breast cancer patients. Pathological evaluation of a suspected breast abnormality requires:
Core biopsy obtained with a needle (core needle biopsy) is the current standard of care for initial confirmation of diagnosis. It has the following advantages over FNAC:
However, FNAC is still highly relevant in settings with limited resources. Most lesions detected in such settings are clinically palpable and studies have shown that the sensitivity and specificity of FNAC from such lesions is marginally lower than that of core biopsy. Moreover, FNAC is rapid, logistically simpler, and can be organized in secondary care facilities. The patient does not have to travel to a tertiary care facility for the confirmation of diagnosis. This avoids any delay in diagnosis. The advantages and disadvantages of the two techniques are compared in detail in the following table. Comparison of FNAC and core needle biopsy as a diagnostic modality:
The next few sections of the atlas deal with both breast cytopathology and histopathology. We will discuss the techniques of sample collection and handling, fixation, processing, and reporting. The atlas does not intend to deal with the interpretation of abnormal findings on cytology and histopathology in detail. That is in the domain of a trained pathologist. |


Click on the pictures to magnify and display the legends
Click on this icon to display a case study
25 avenue Tony Garnier CS 90627 69366, LYON CEDEX 07 France - Tel: +33 (0)4 72 73 84 85
© IARC 2025 - Terms of use - Privacy Policy.
© IARC 2025 - Terms of use - Privacy Policy.