



Home / Training / Manuals / Atlas of breast cancer early detection / Learning
.png)
Click on the pictures to magnify and display the legends

Click on this icon to display a case study
Atlas of breast cancer early detection
Filter by language: English / РусскийBreast imaging Mammography interpretation Mammography lexicon Calcifications Typically benign calcifications |
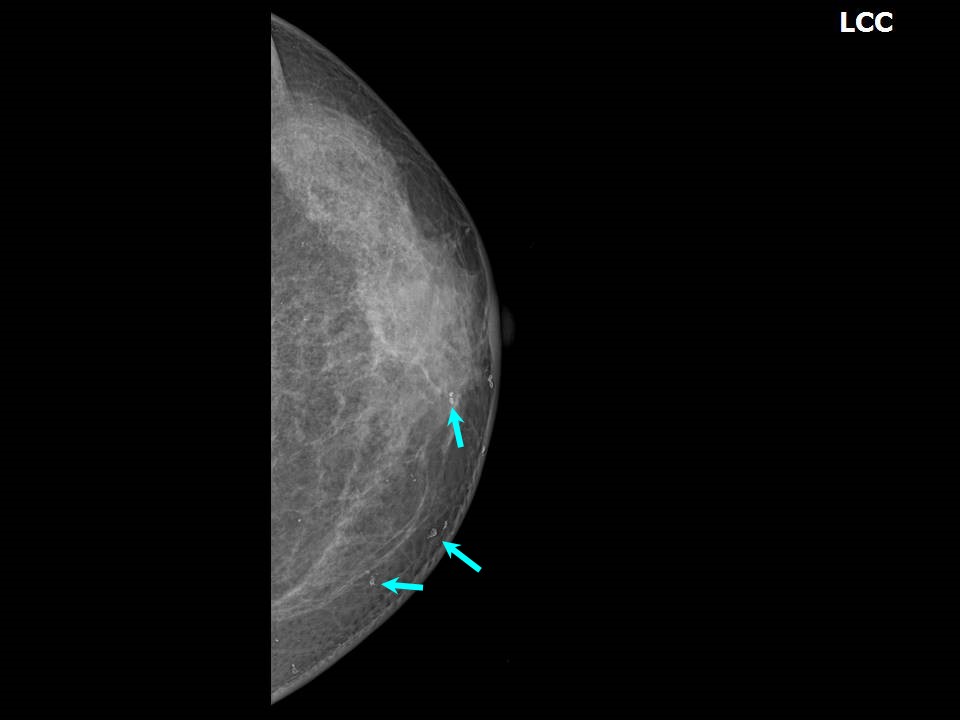
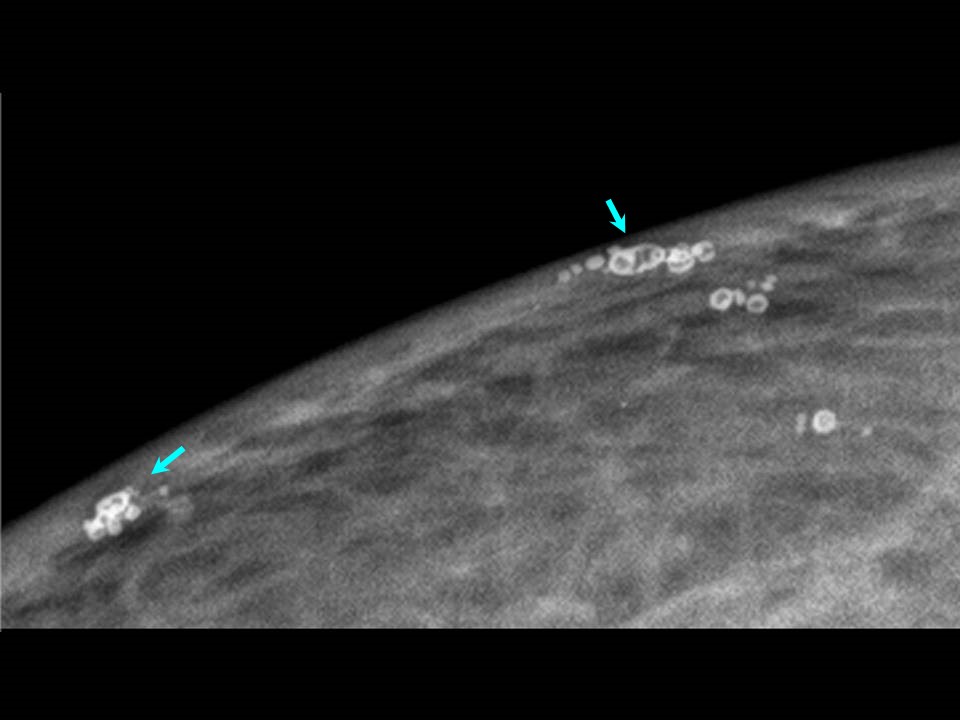
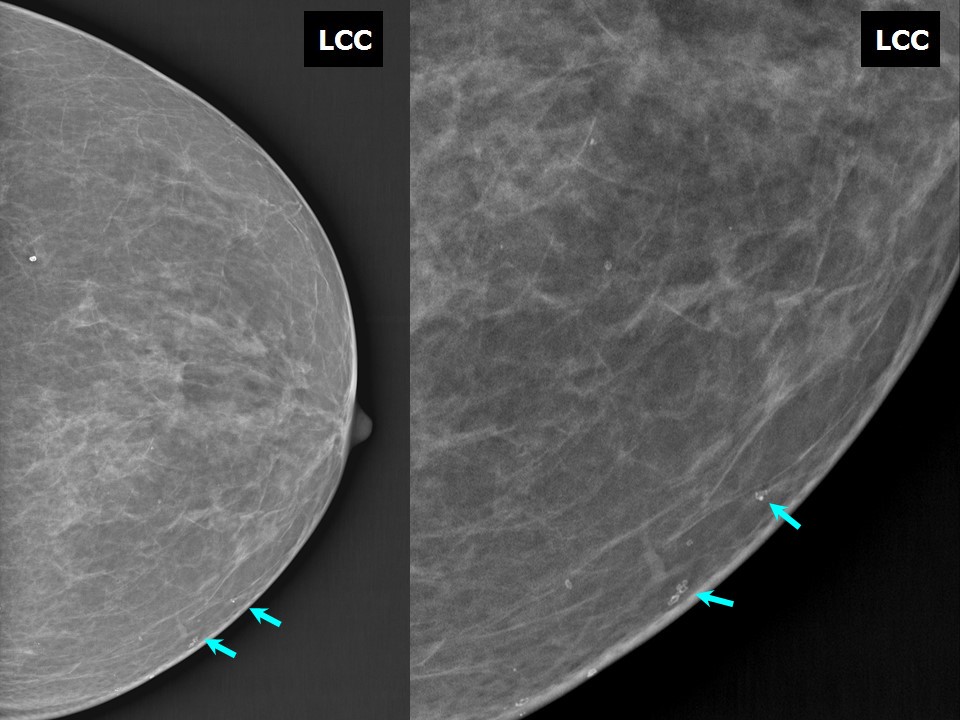
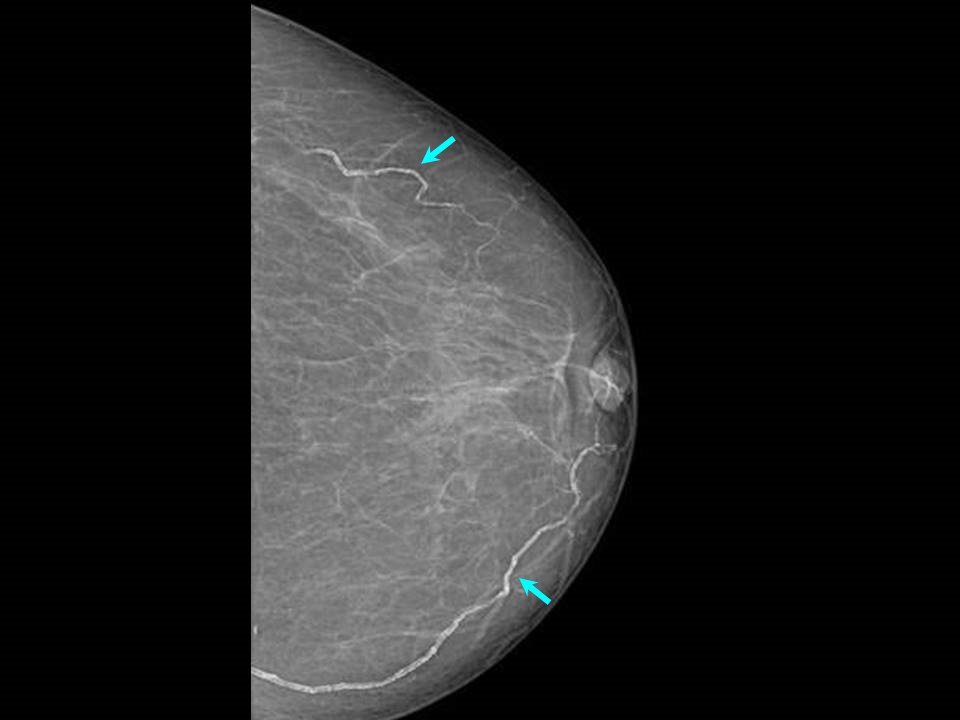
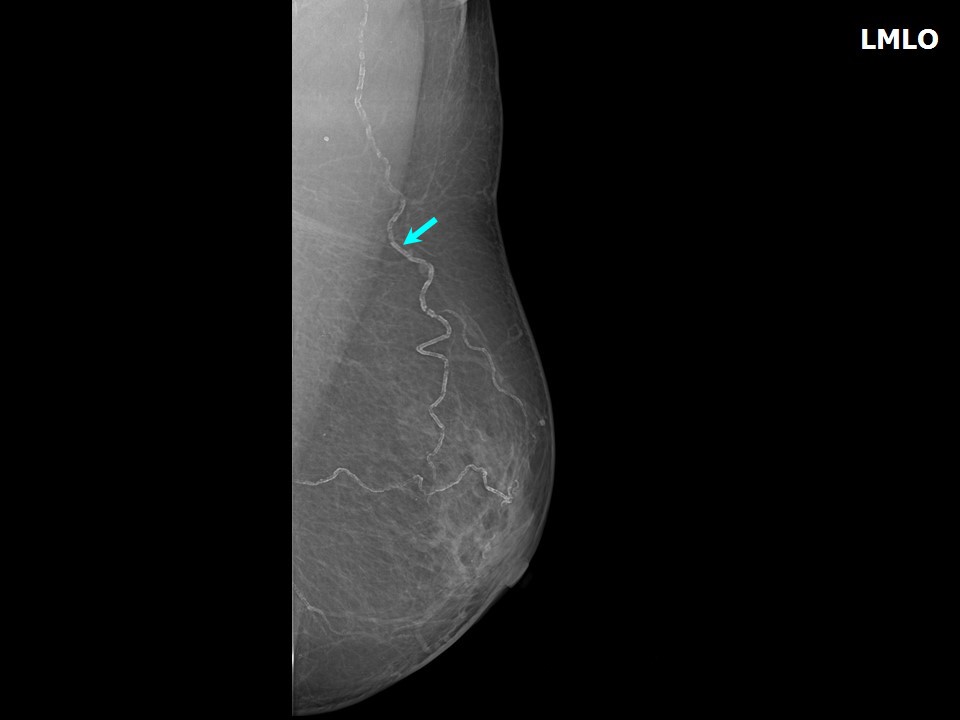
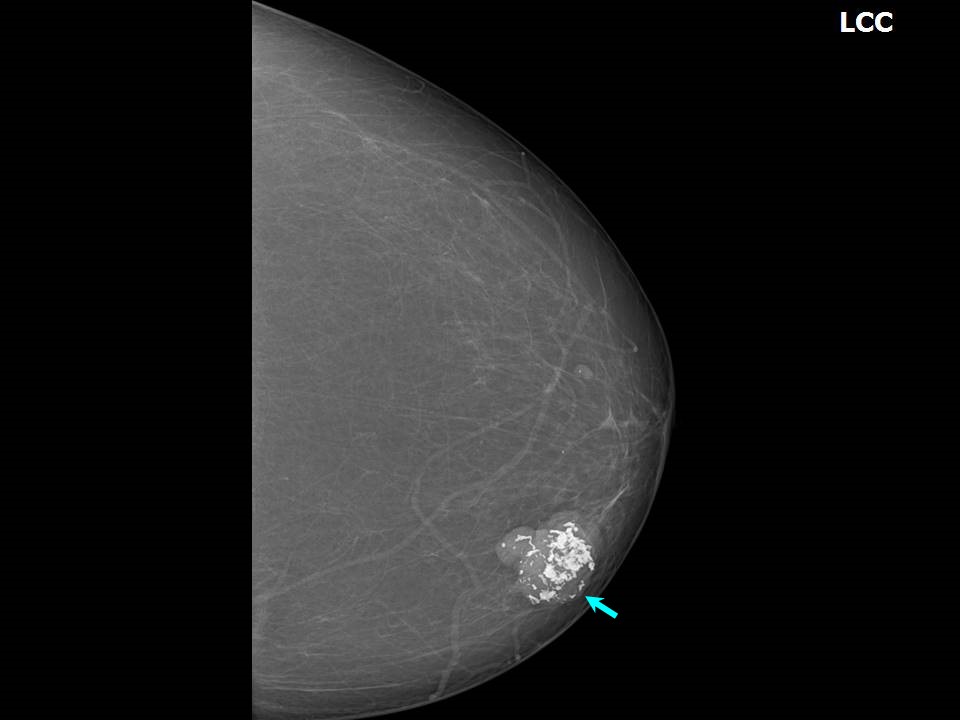
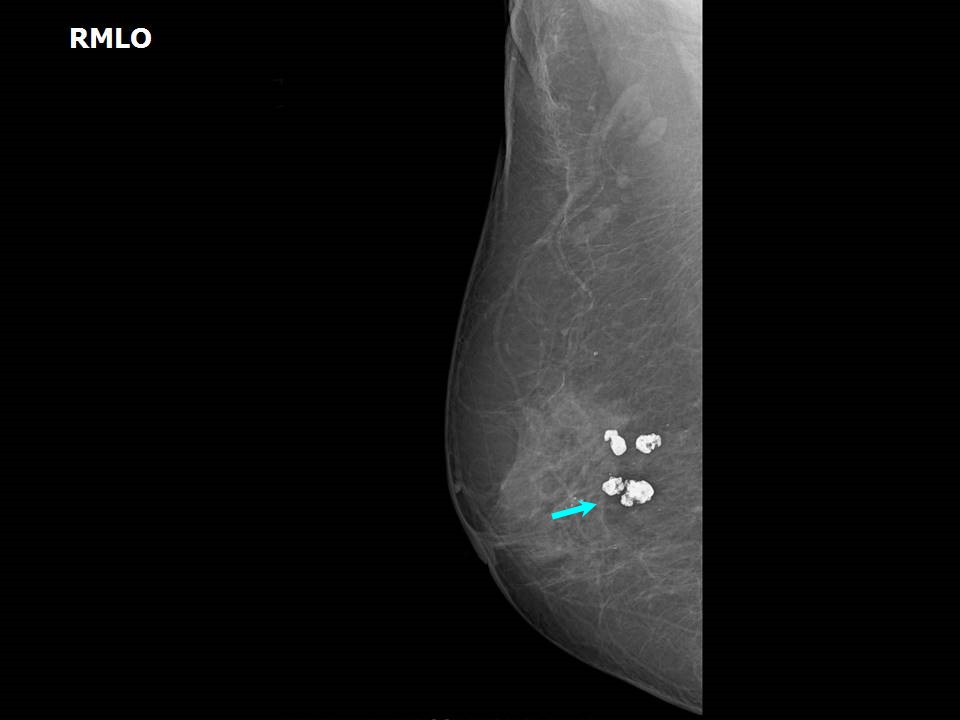
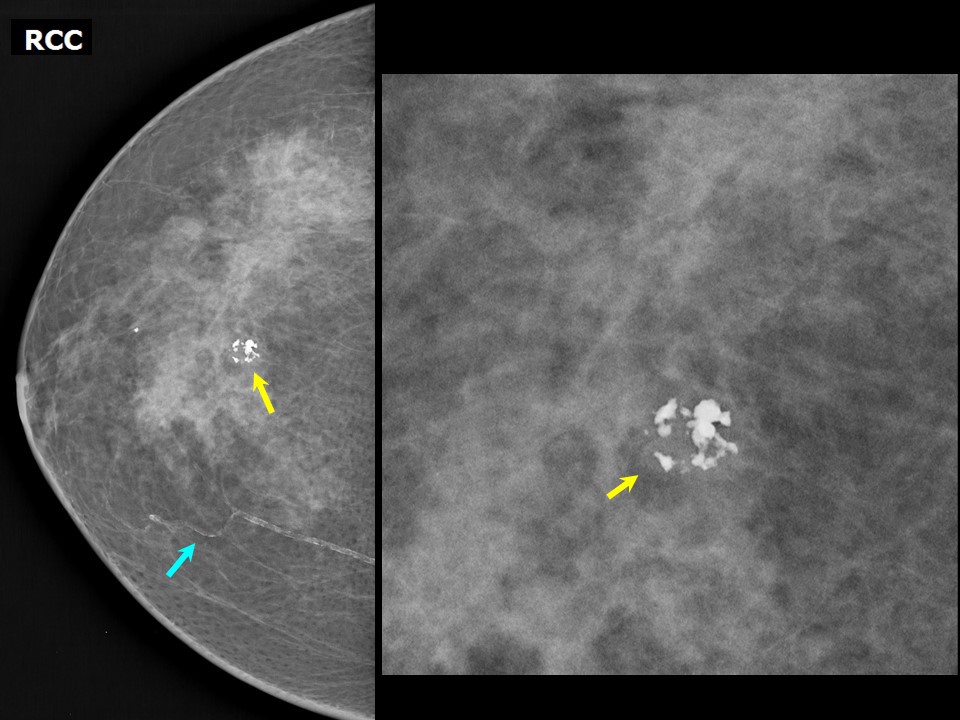
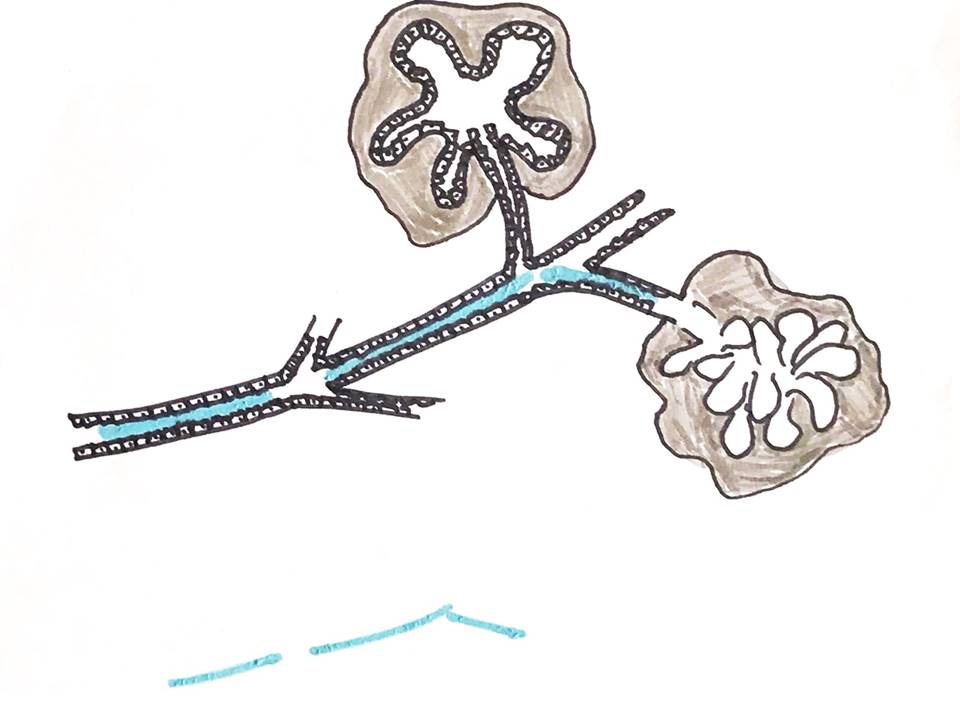
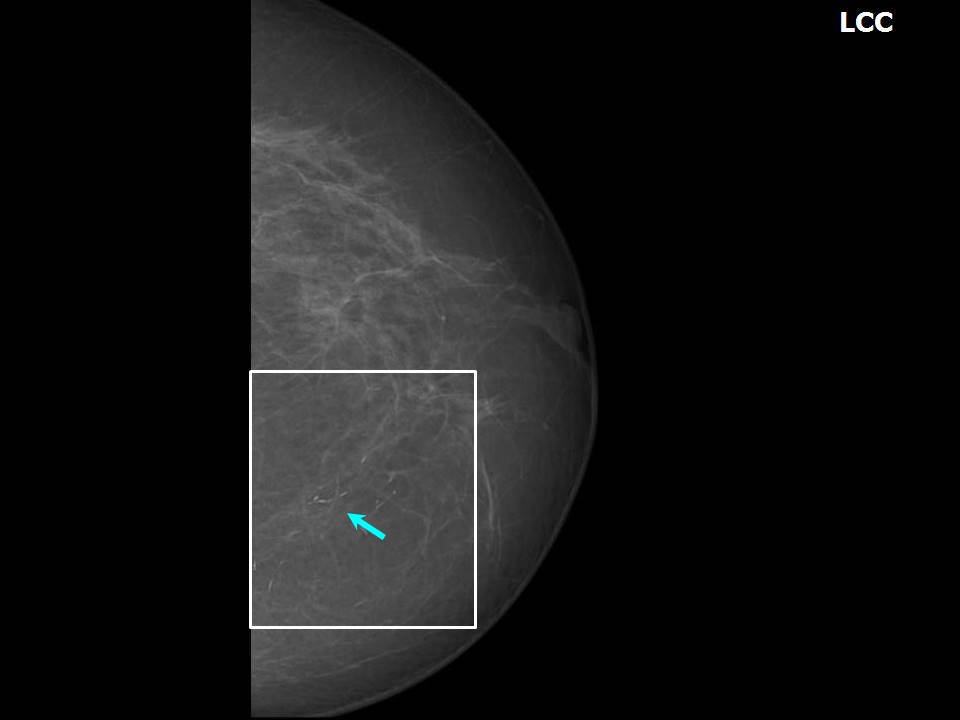
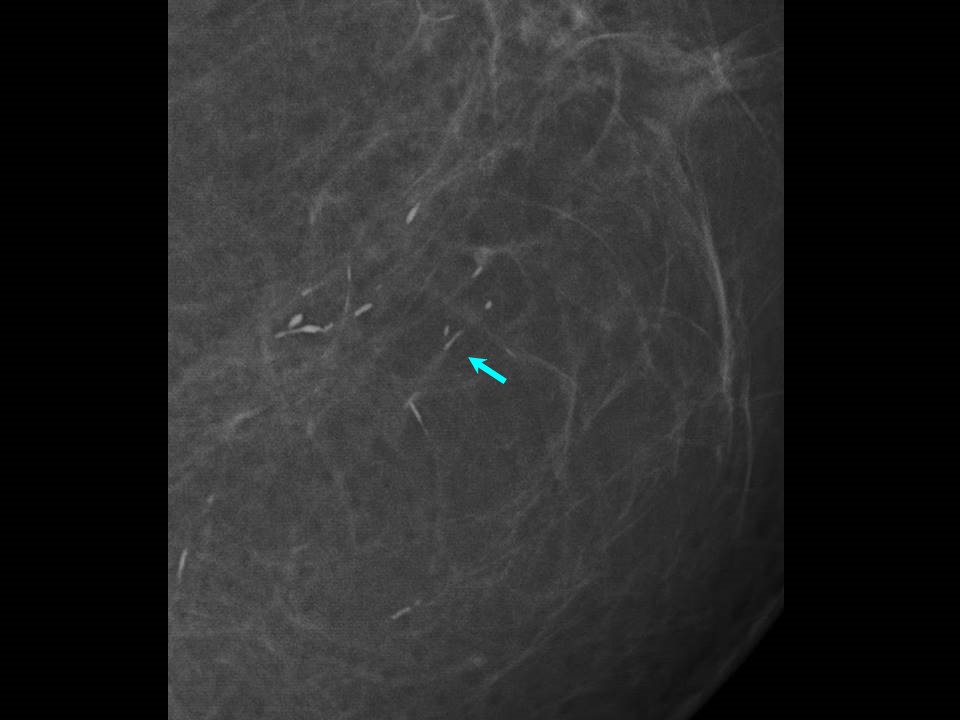
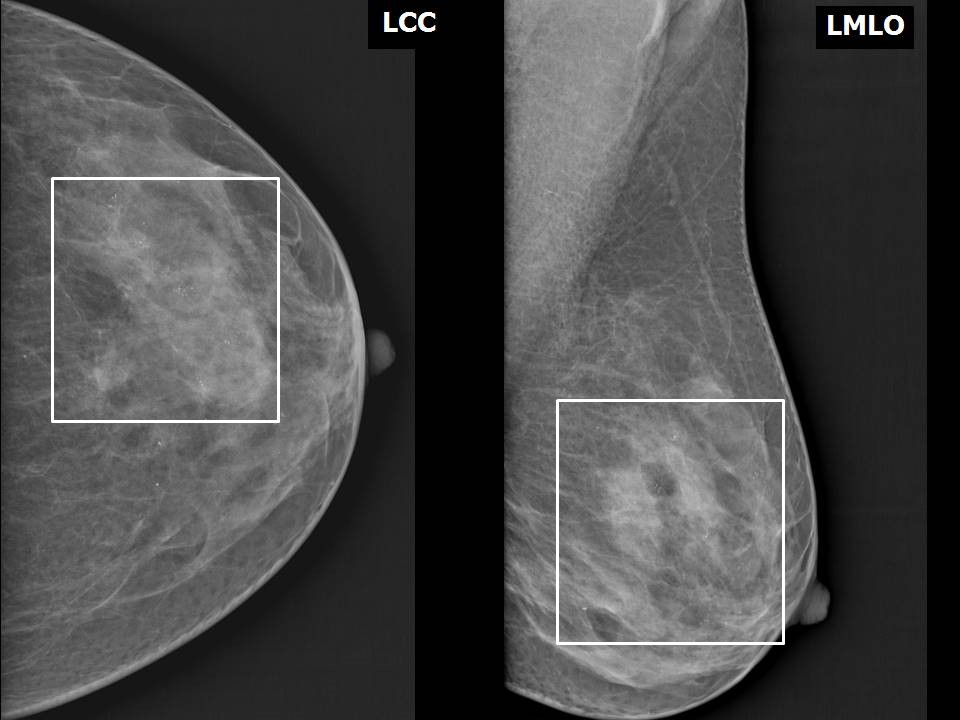
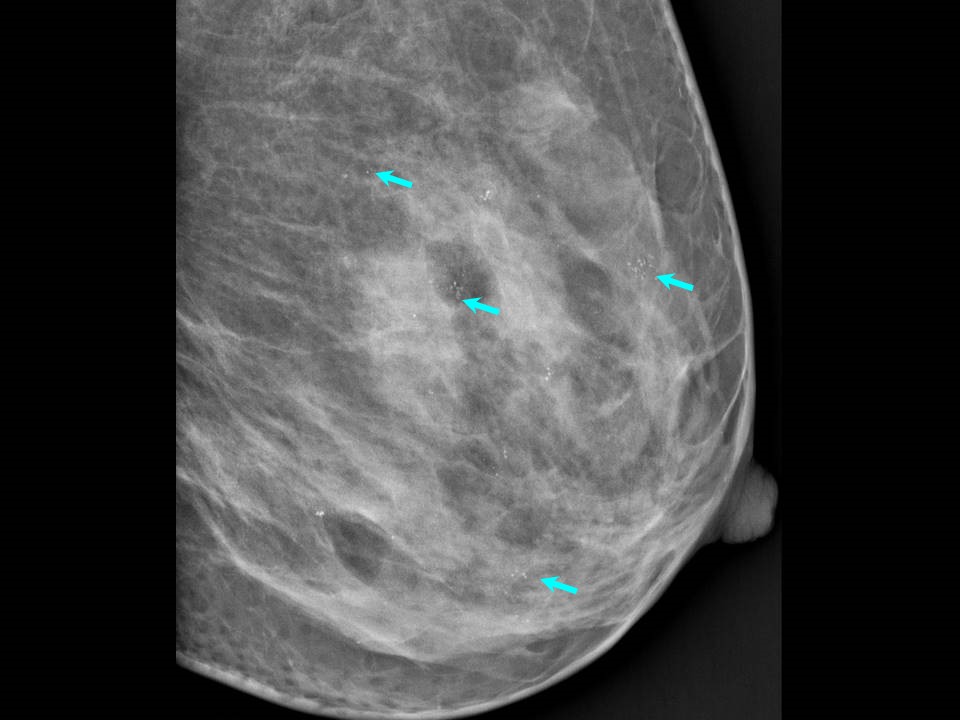
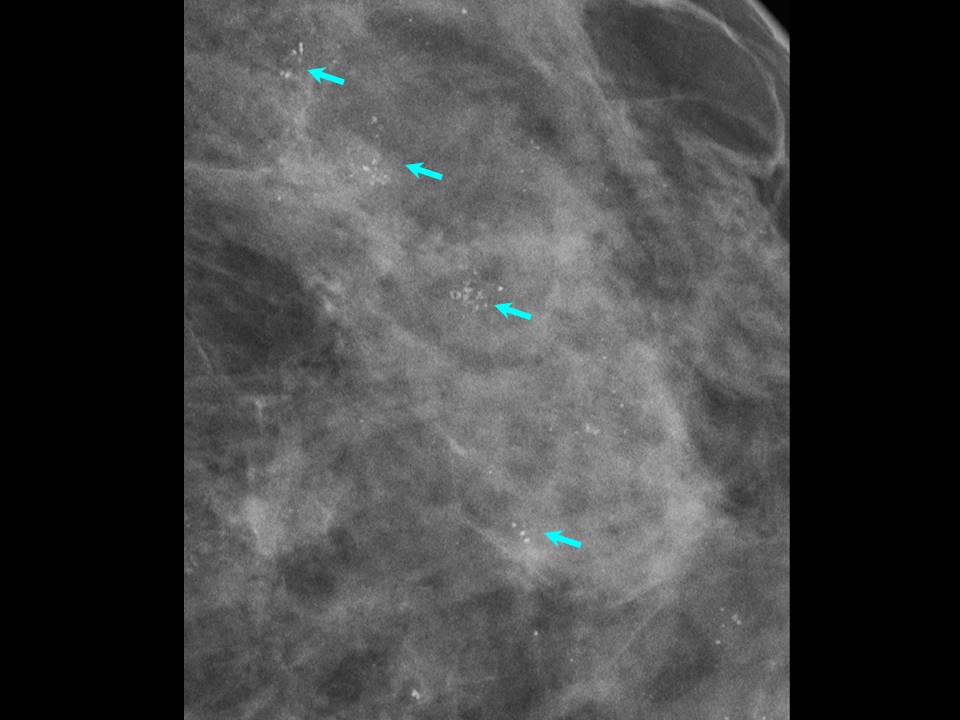
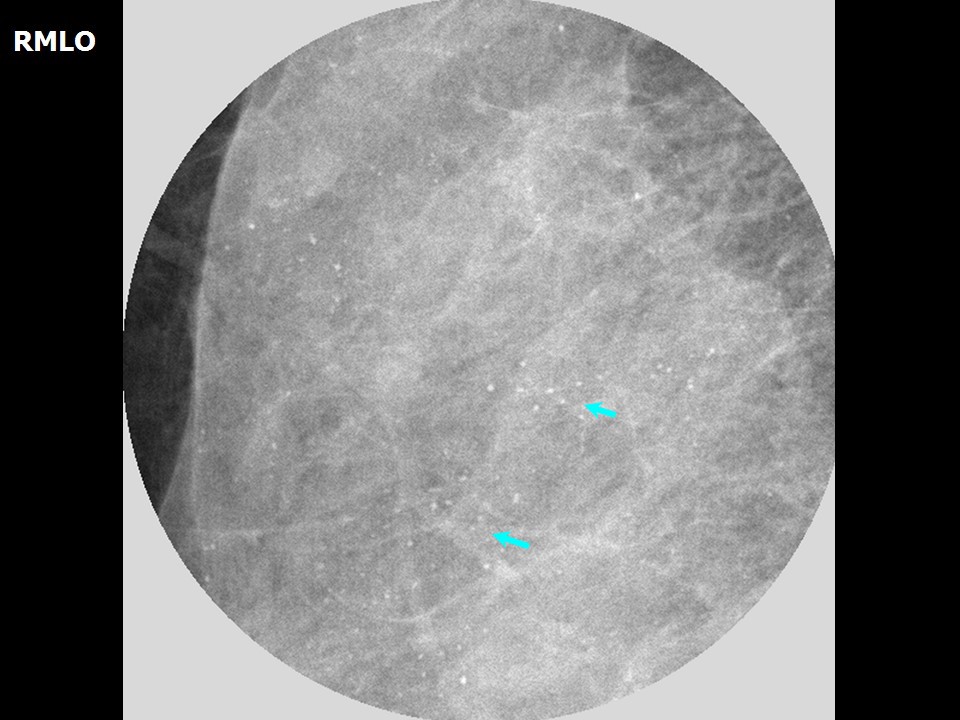
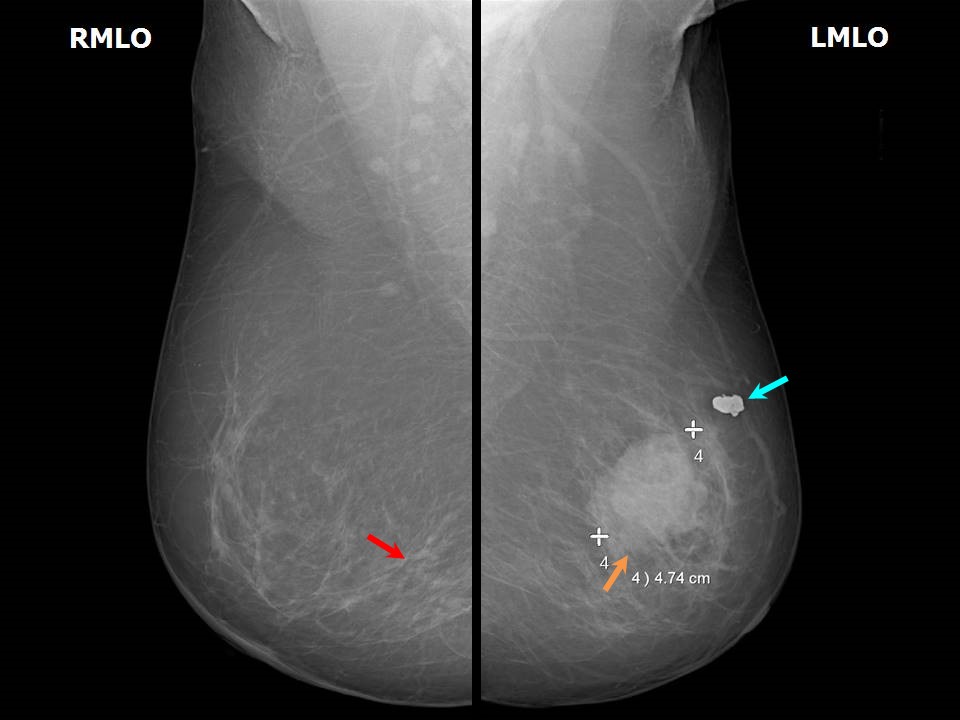
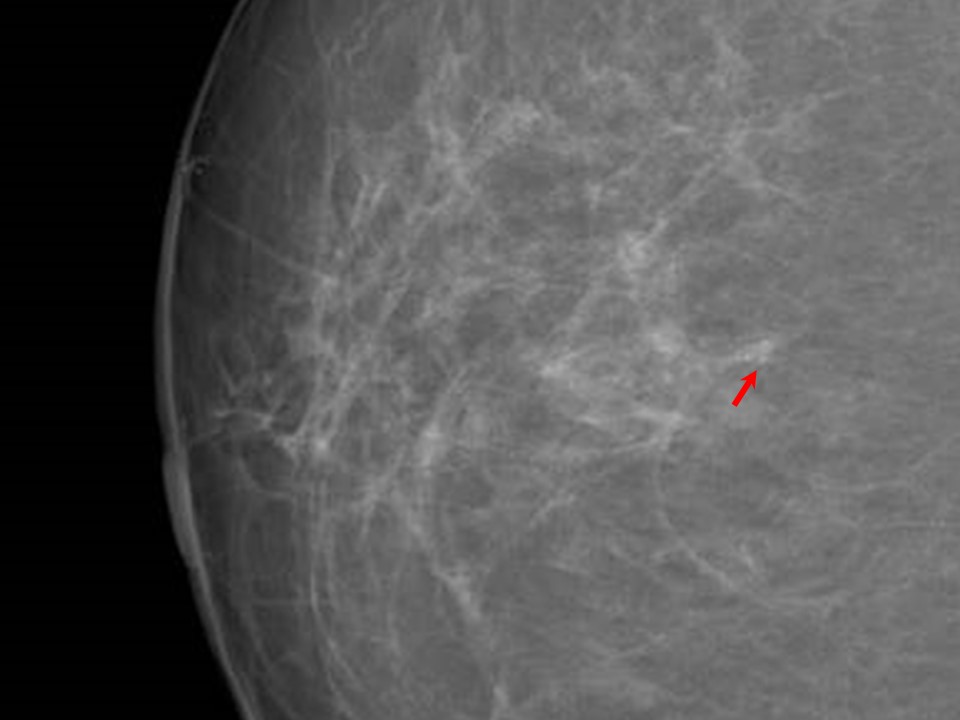
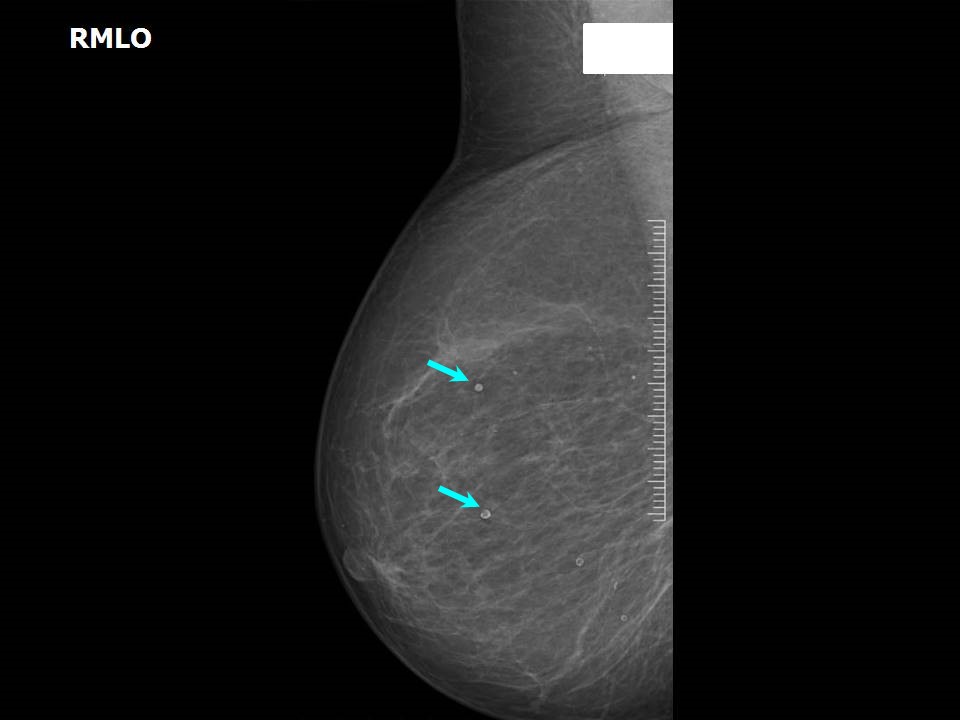
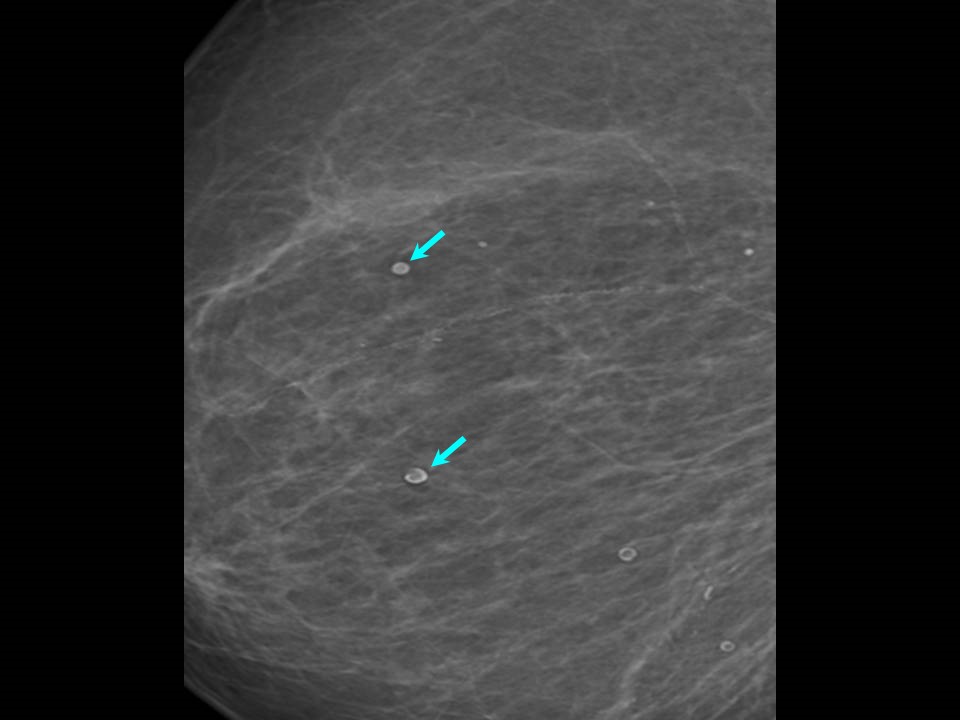
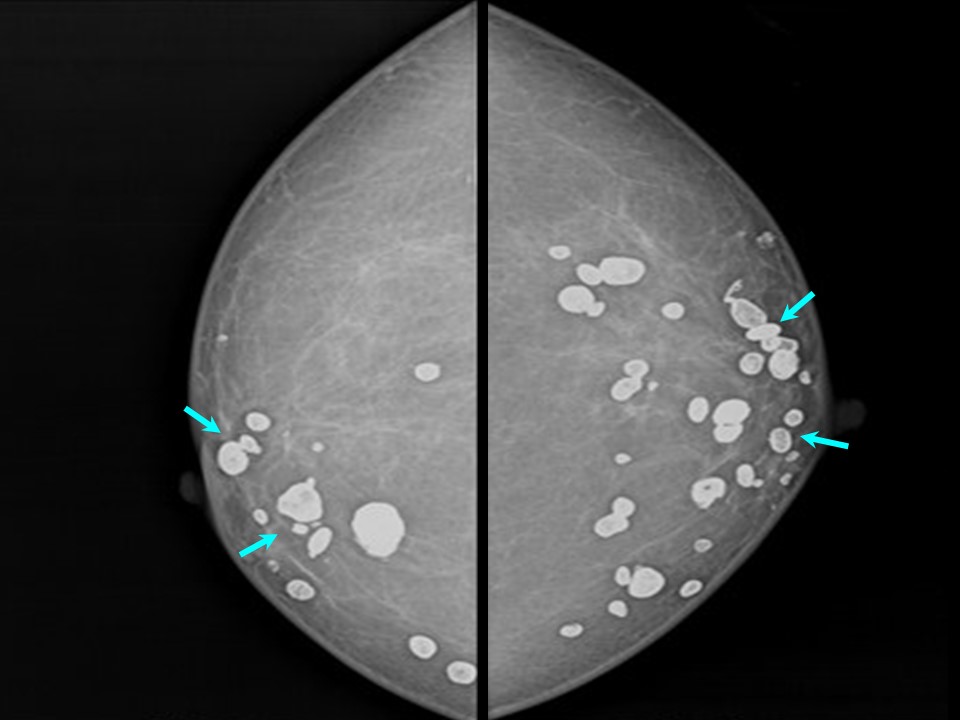
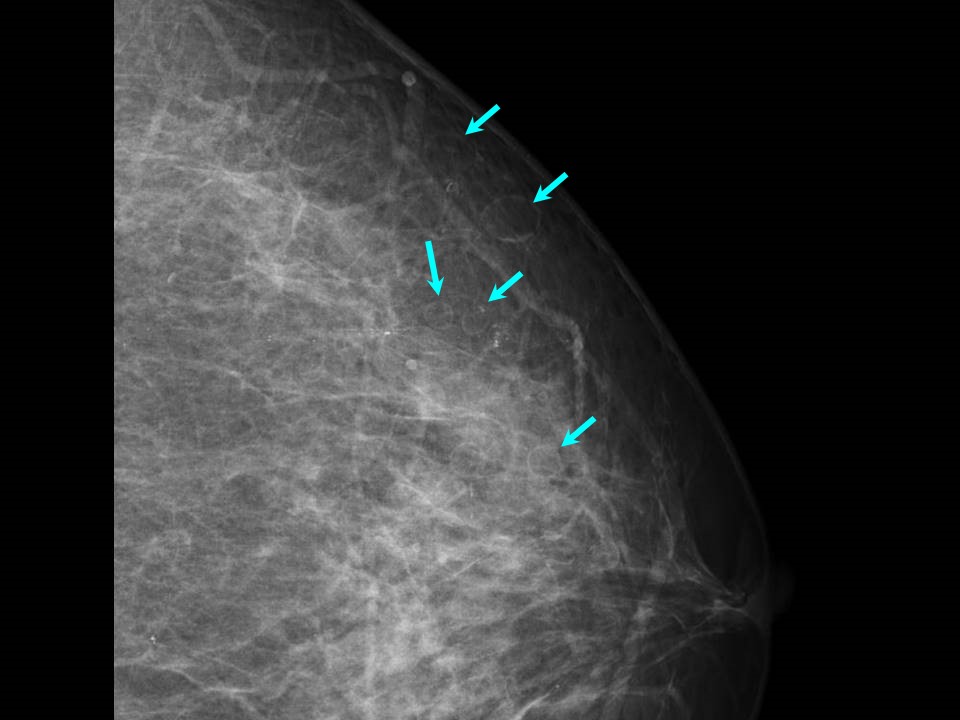
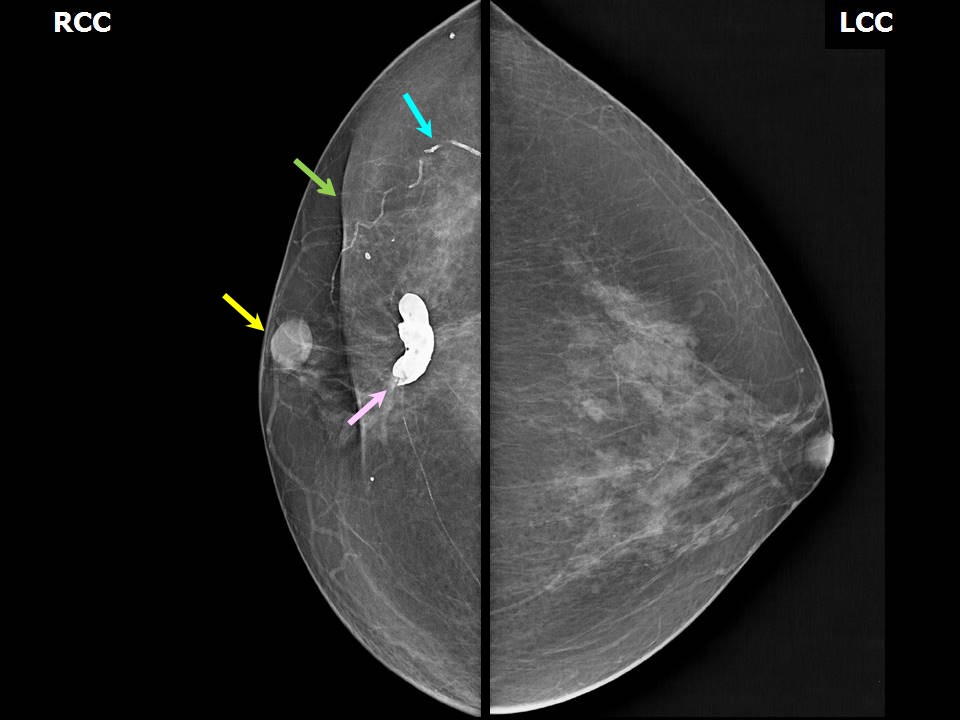
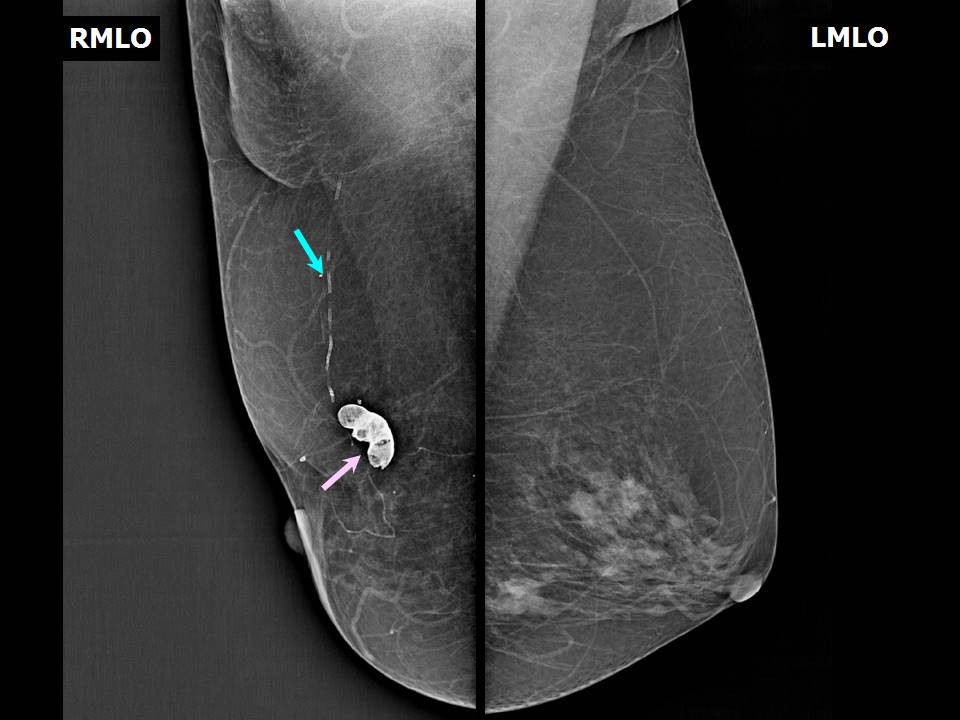
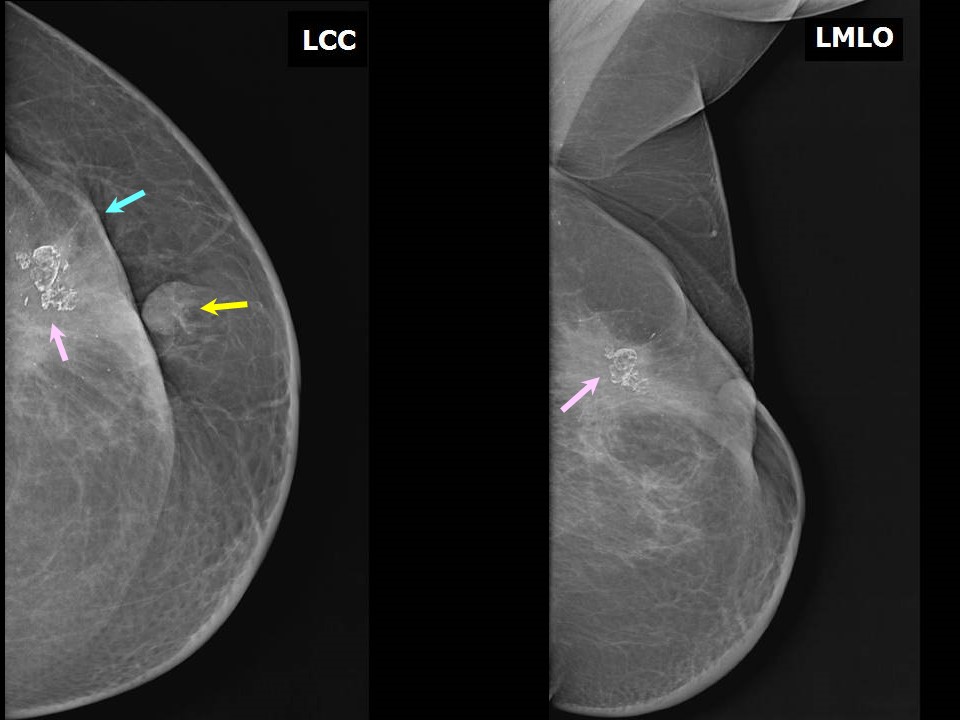
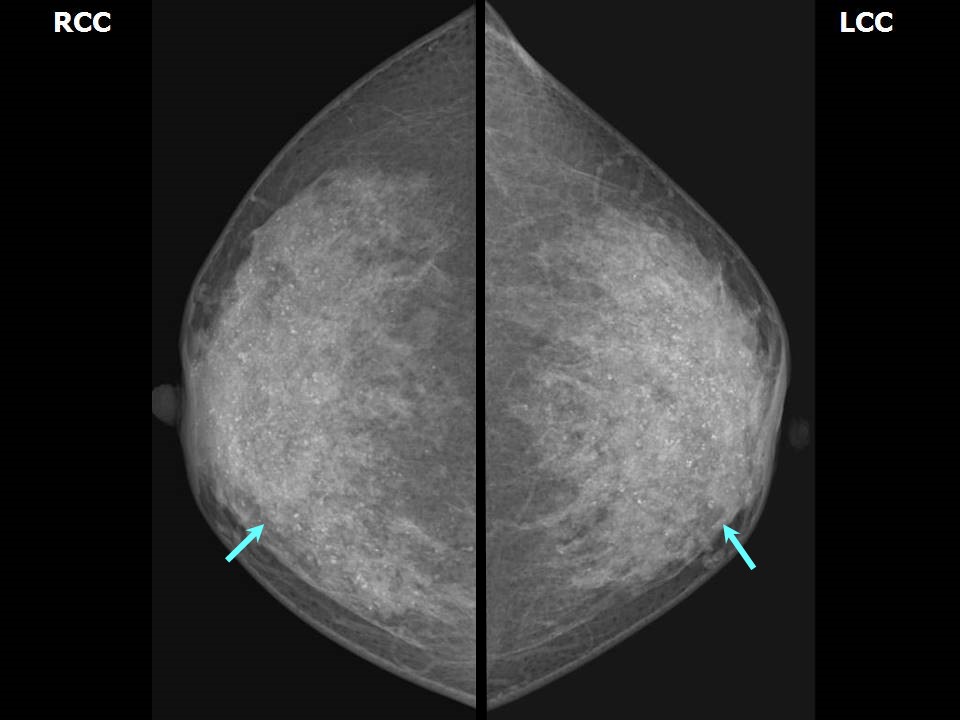
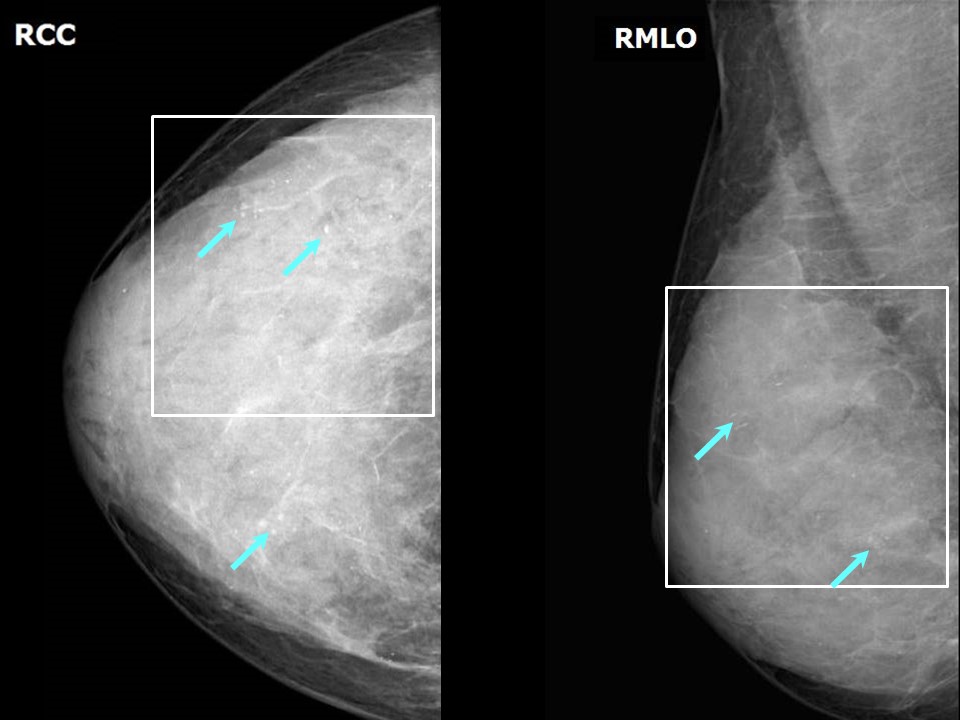
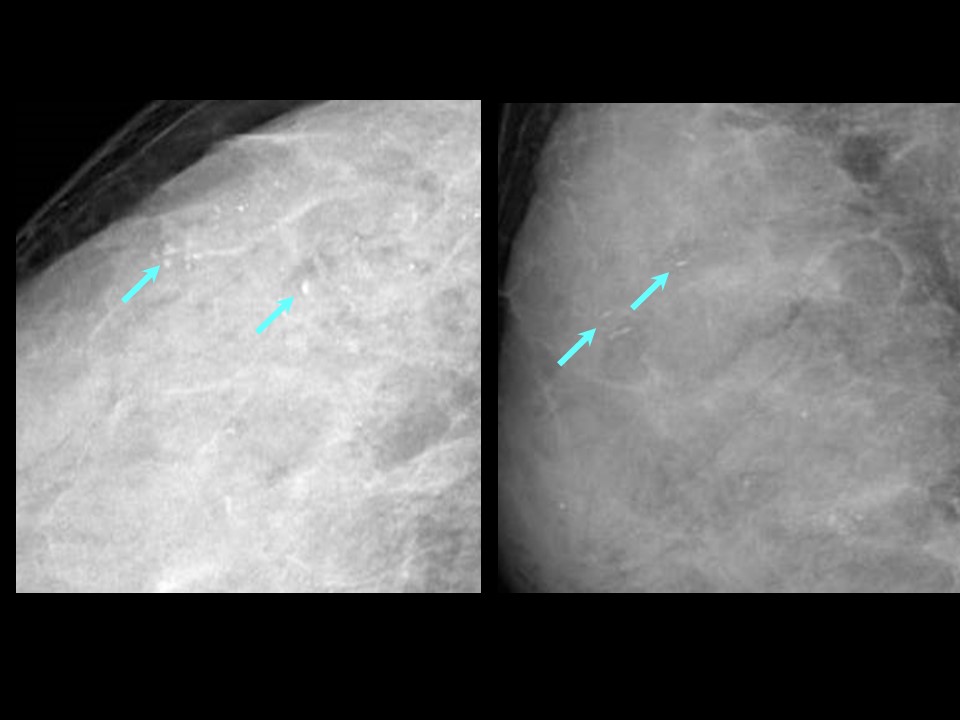
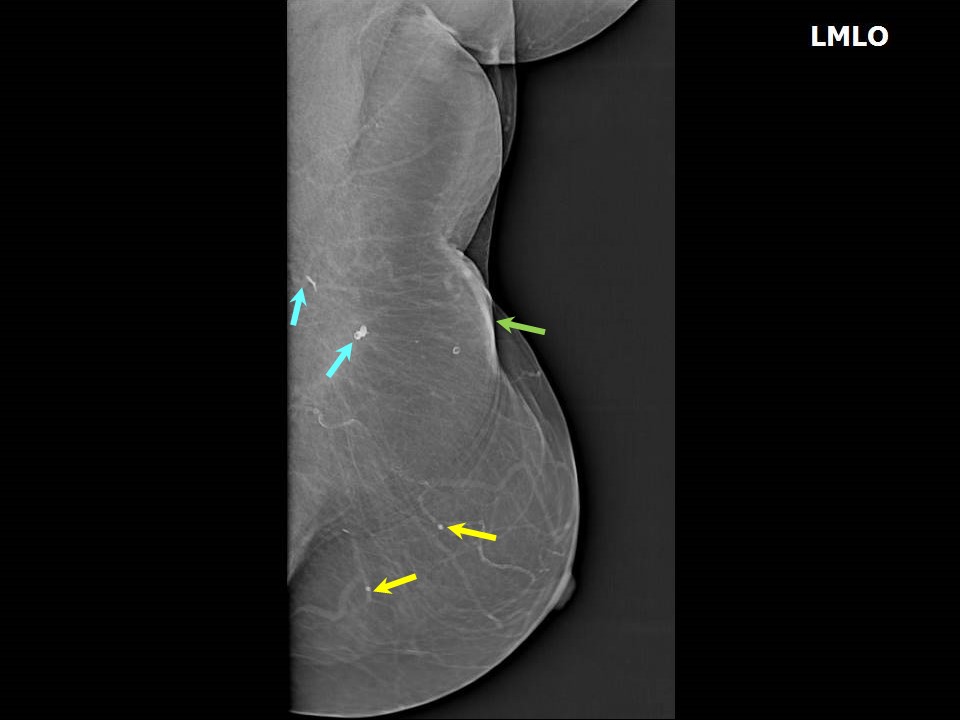
The breast calcifications visualized on mammography are further categorized by their morphology and distribution according to the BI-RADS lexicon. 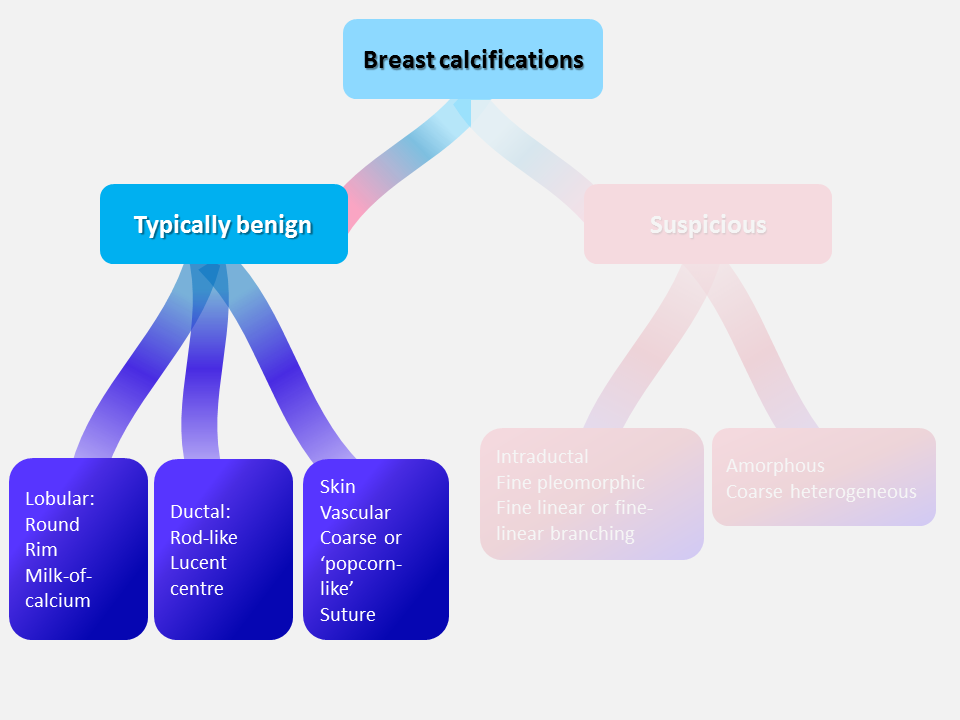 Typically benign This morphological category includes the following subtypes. Skin calcifications These are very common, usually lucent-centred deposits with diffuse distribution over the breasts. They are more commonly seen along the sternal side .Vascular calcifications These form in the walls of blood vessels and are seen as linear parallel track-like calcifications. Early vessel calcifications may look like linear branching calcifications .Spot compression magnification mammography is helpful to characterize these calcifications. Malignant calcifications form within dead cancer cells debris in the duct lumen and are seen as a single line. Coarse or popcorn-like calcifications Typically benign large popcorn-like calcifications are produced by involuting fibroadenomas. These calcifications do not usually cause a diagnostic problem and are of no concern .Large rod-like calcifications These are seen as continuous rods that branch in ductal distribution and radiate towards the nipple. They are benign calcifications that form within ectatic ducts. The calcified streaks are thicker, usually > 1 mm in diameter, and have sharp margins. They are usually bilateral and are most often seen in women older than 60 years .Round calcifications Round calcifications 0.51 mm across form in the cystically dilated acini of the TDLUs and are thus called acinar or lobular calcifications .Round calcifications are categorized as either diffuse or grouped according to their arrangement. Diffuse round calcifications These are typically benign calcifications, seen in fibrocystic changes, adenosis, or skin calcification. Grouped (clustered) round calcifications Round calcifications are classified as grouped/clustered calcifications if there are at least five calcifications within 1 cm of each other or if there are numerous calcifications within 2 cm of each other. These calcifications are suspicious and should be followed up to ascertain stability. Rim calcifications These are subcategorized as lucent-centred or eggshell calcifications. Lucent-centred calcifications are round or oval calcifications that are < 1 mm to > 1 cm in greatest dimension. They usually form as a result of fat necrosis or calcified debris in ducts and are less often seen in fibroadenoma. Eggshell calcifications are benign calcifications that are very thin, usually < 1 mm thick and are formed as a result of calcium deposited on the surface of a sphere. They are commonly seen as calcifications in the wall of cysts .Dystrophic calcifications Dystrophic calcifications are > 0.5 mm in greatest dimension, coarse and irregular in shape, often with lucent centres, and have a typically crushed lava appearance. They are seen adjacent to scars in women who have undergone lumpectomy and radiotherapy. These fat necrosis calcifications develop 35 years after treatment in about 30% of patients .Milk of calcium calcifications Milk of calcium calcifications are benign lobular calcifications that are seen as indistinct and fuzzy round or amorphous calcifications sedimented within the macro or microcysts of the lobules .Suture calcifications Suture calcifications are calcium deposits on postoperative suture material probably due to delayed resorption of the sutures. Calcium can deposits directly in the scar, the oleogranulemas can be appear. They are seen as typically linear or tubular calcifications. In some cases, knots may be visible . |






Click on the pictures to magnify and display the legends
Click on this icon to display a case study
25 avenue Tony Garnier CS 90627 69366, LYON CEDEX 07 France - Tel: +33 (0)4 72 73 84 85
© IARC 2025 - Terms of use - Privacy Policy.
© IARC 2025 - Terms of use - Privacy Policy.