



Home / Training / Manuals / Atlas of breast cancer early detection / Learning
.png)
Click on the pictures to magnify and display the legends

Click on this icon to display a case study
Atlas of breast cancer early detection
Filter by language: English / РусскийBreast imaging Breast ultrasound Ultrasound lexicon Associated features Duct changes |
The ability of breast ultrasound to detect mammary duct changes has good specificity and sensitivity and can be used for the diagnosis and differential diagnosis of the causes of duct changes.
Normal mammary ducts (1012 in each breast) are seen on ultrasound as fine linear anechoic branching structures, < 2 mm in diameter. Dilated ducts are > 2 mm in diameter. They may be single or multiple, in one or both breasts. Ductal abnormalities are seen as an isolated finding or an associated feature of breast disease. Ductal abnormalities may be physiological changes or pathological findings. Ultrasound has good sensitivity to detect intraductal masses, echoes, or calcifications. Duct changes Duct changes are classed as either isolated findings or associated features.
It is important to detail duct changes when performing a targeted diagnostic or screening ultrasound to differentiate between benign and malignant causes of duct dilatation. The causes may include:
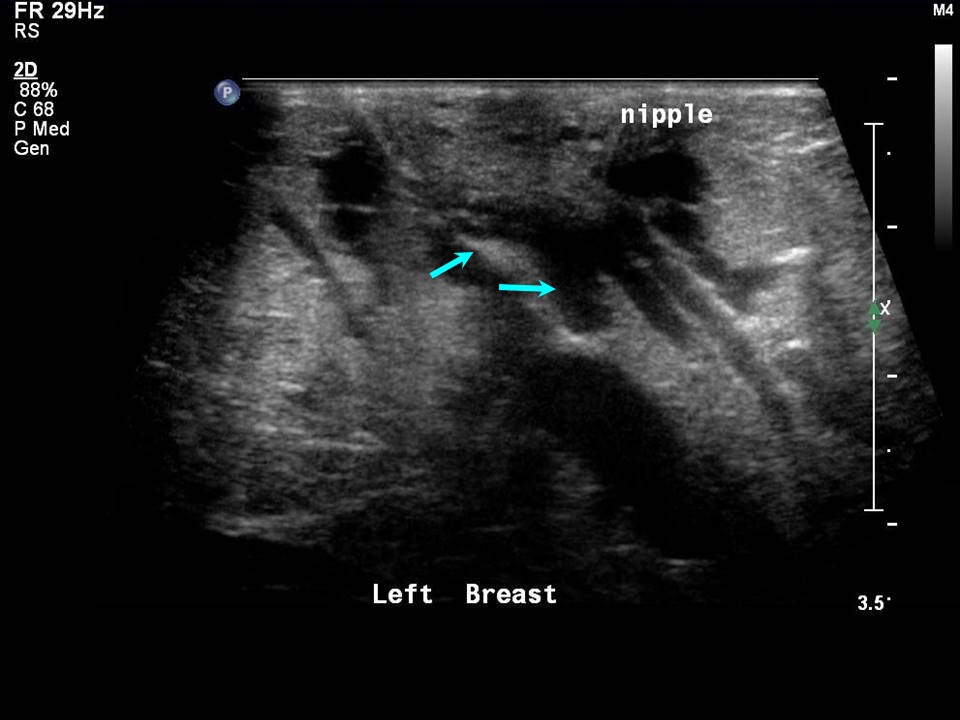
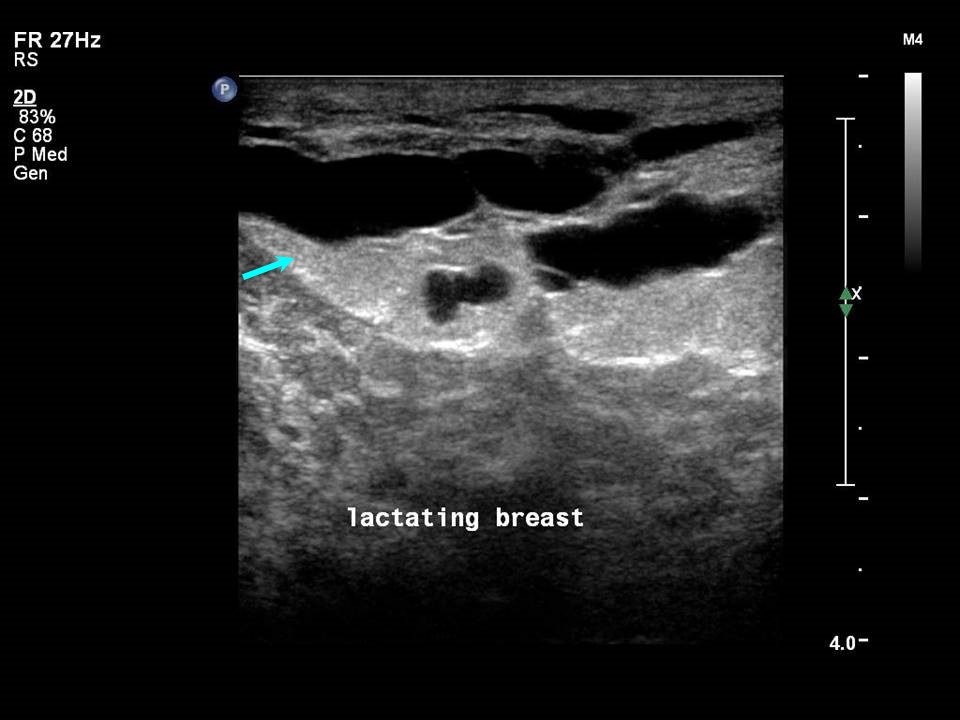
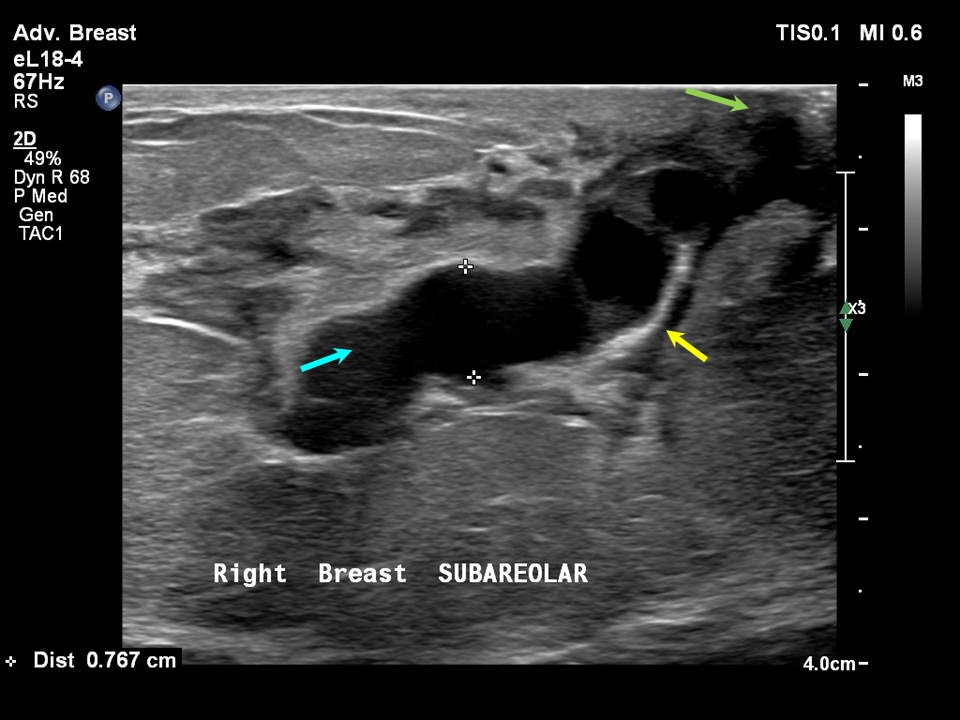
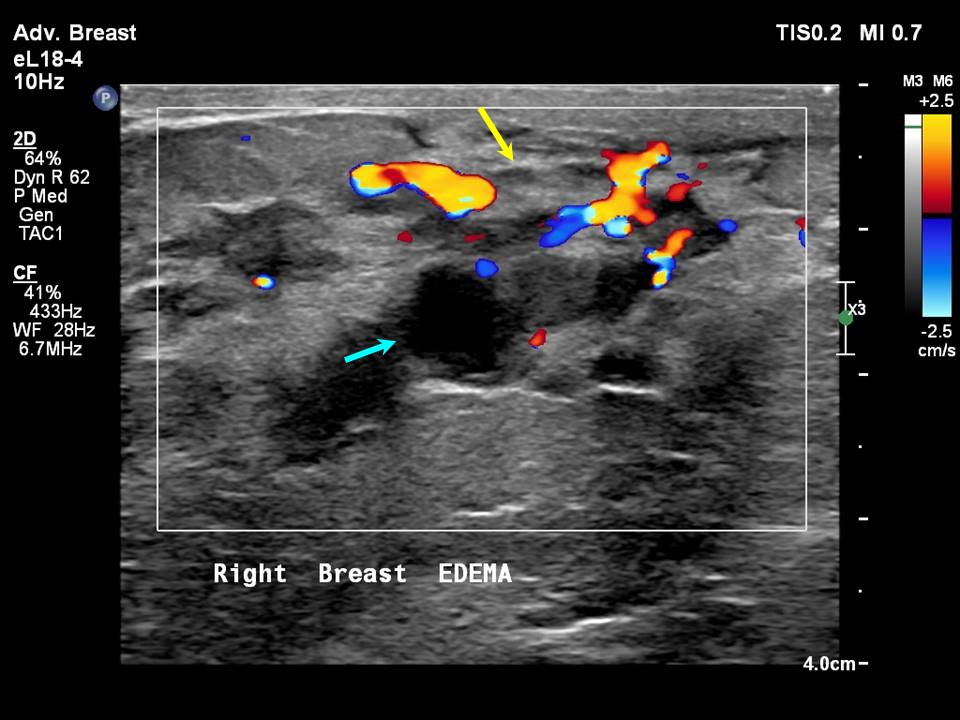
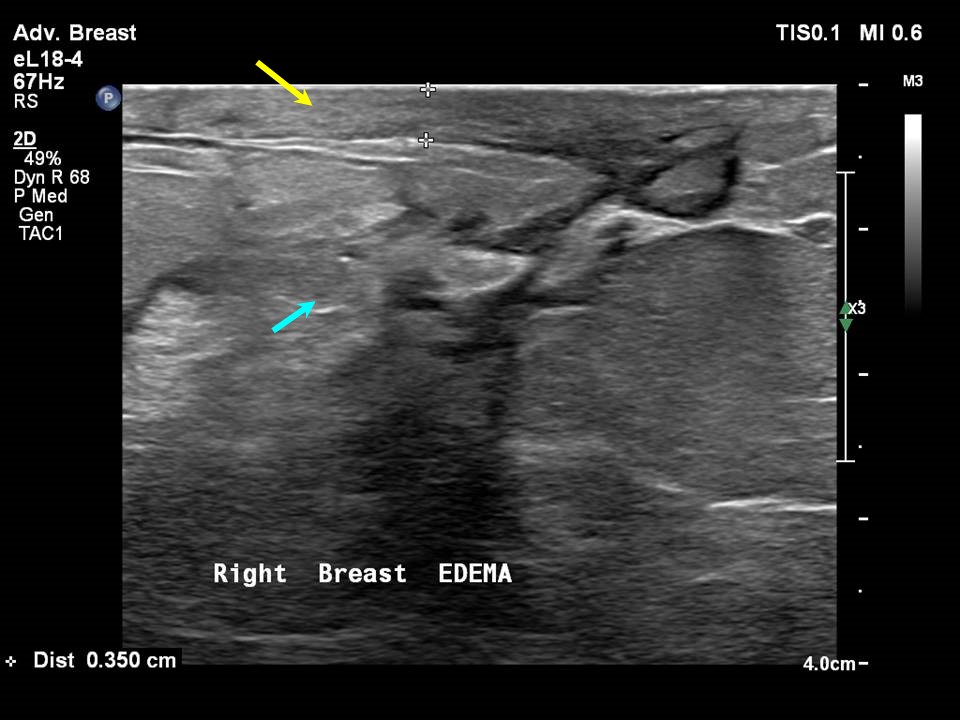
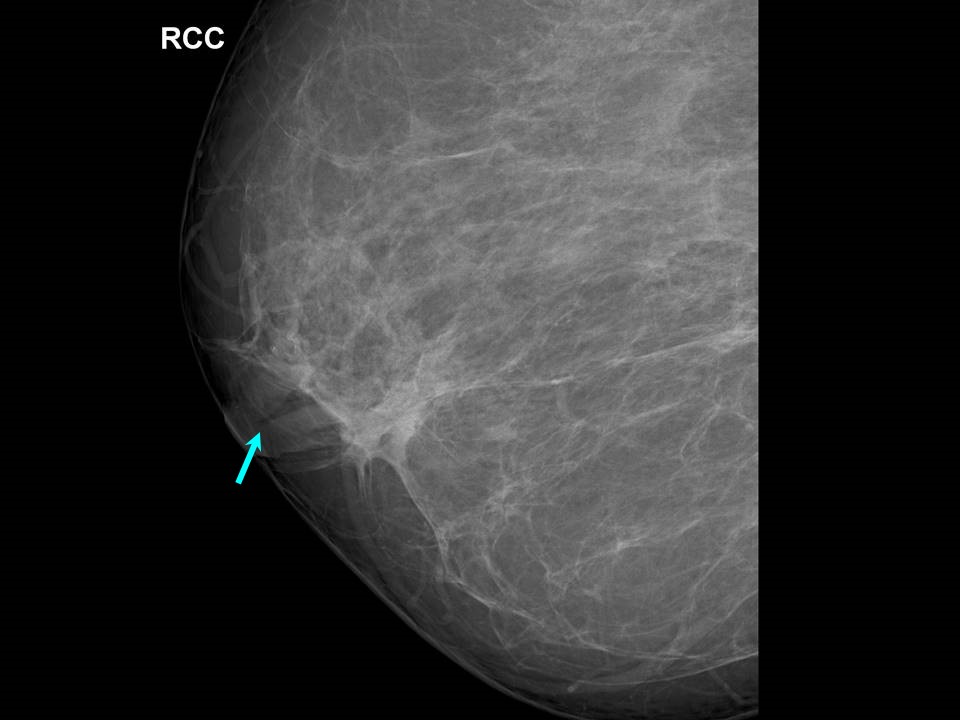
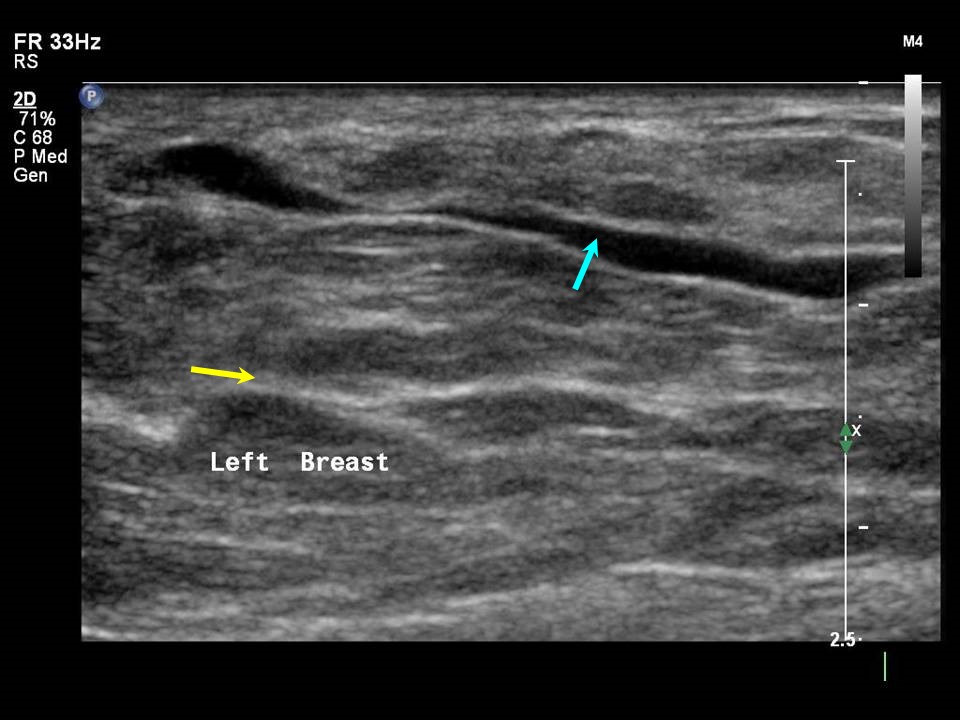
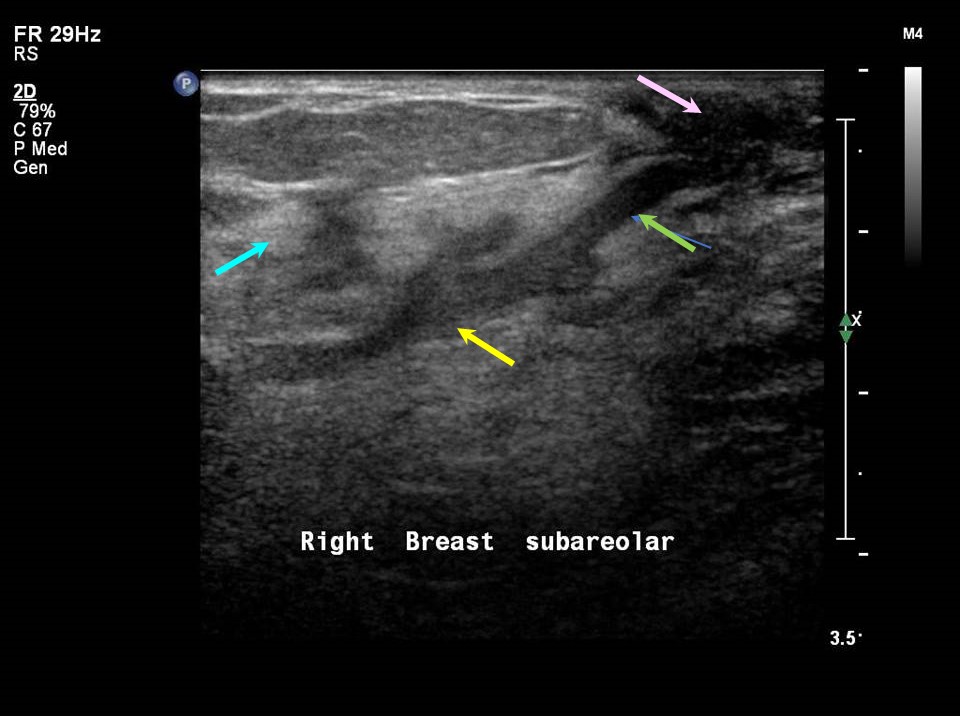
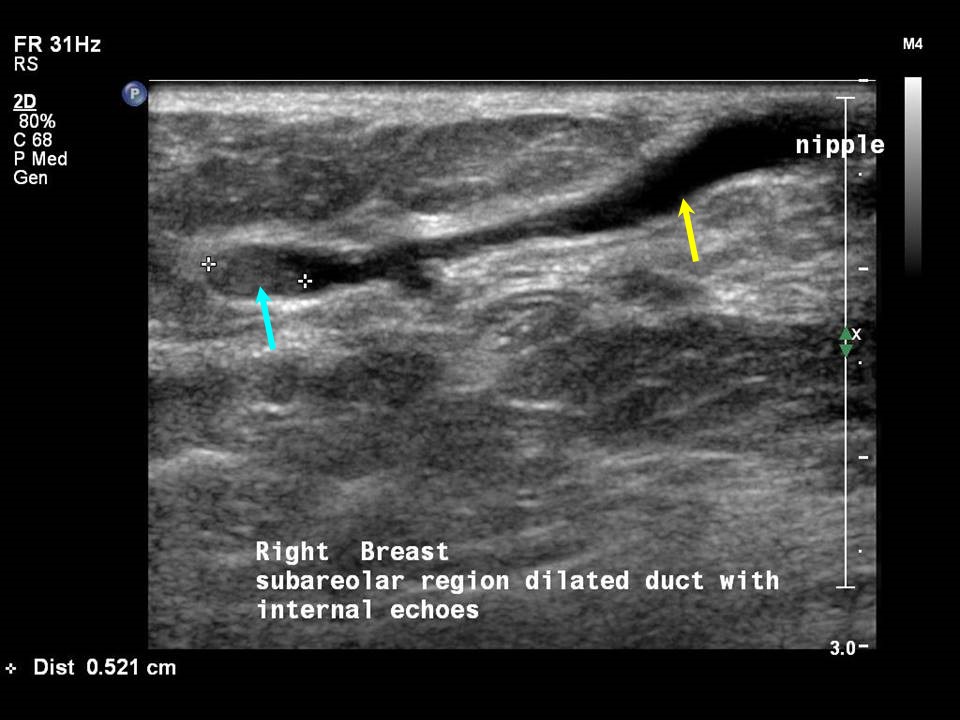
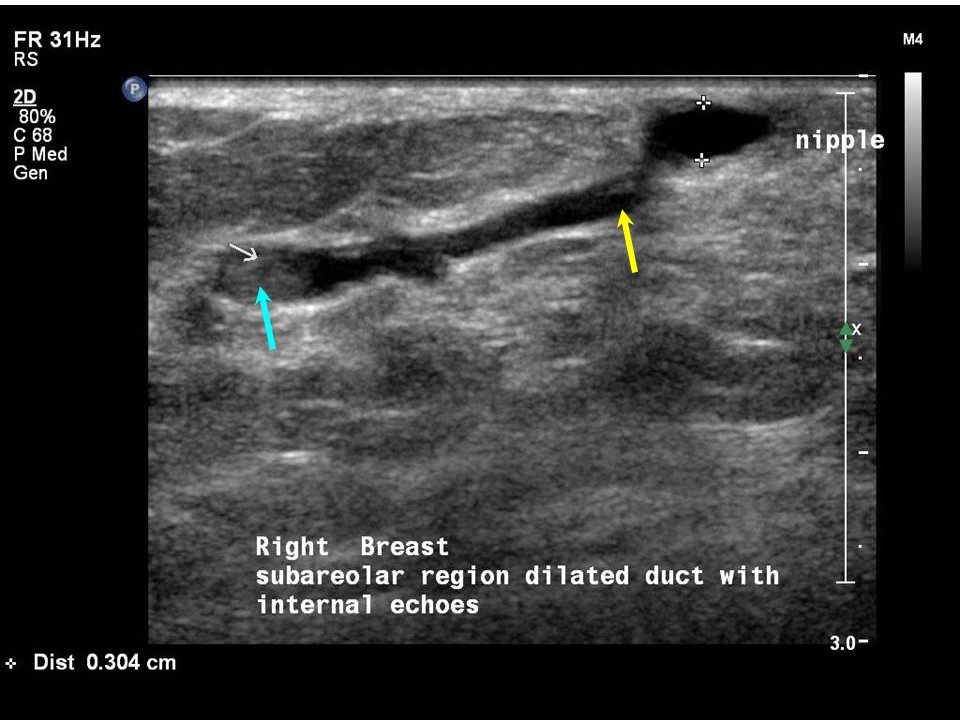
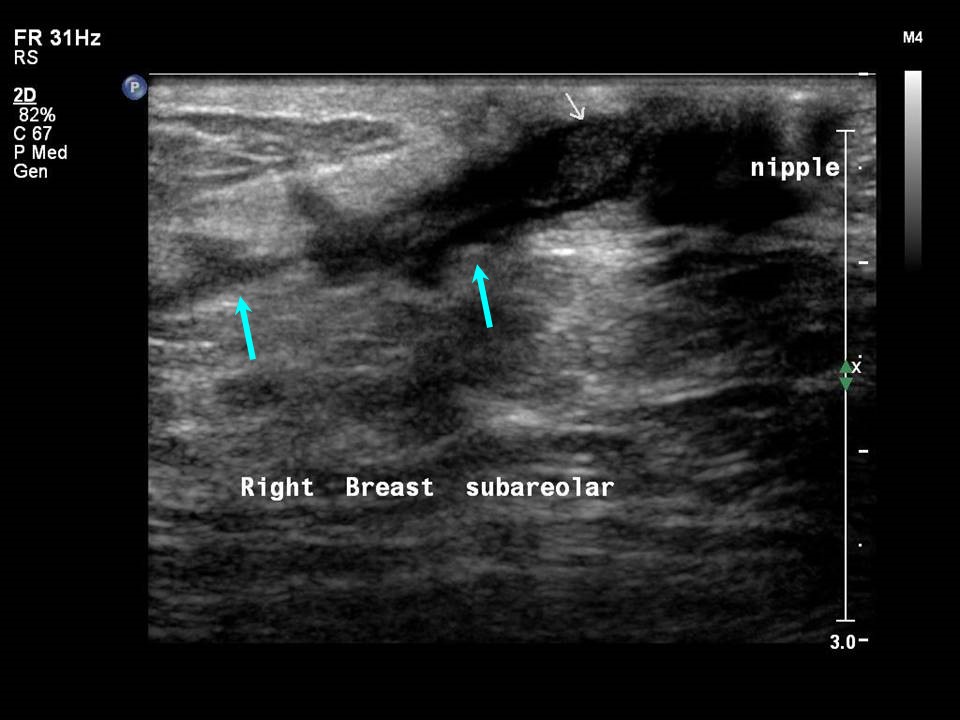
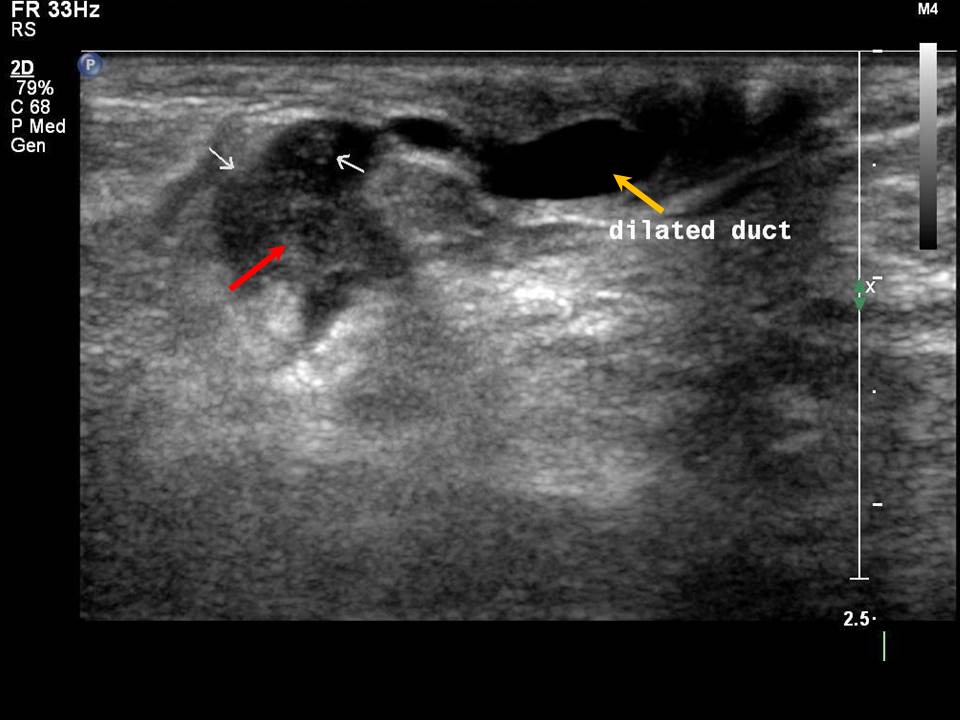
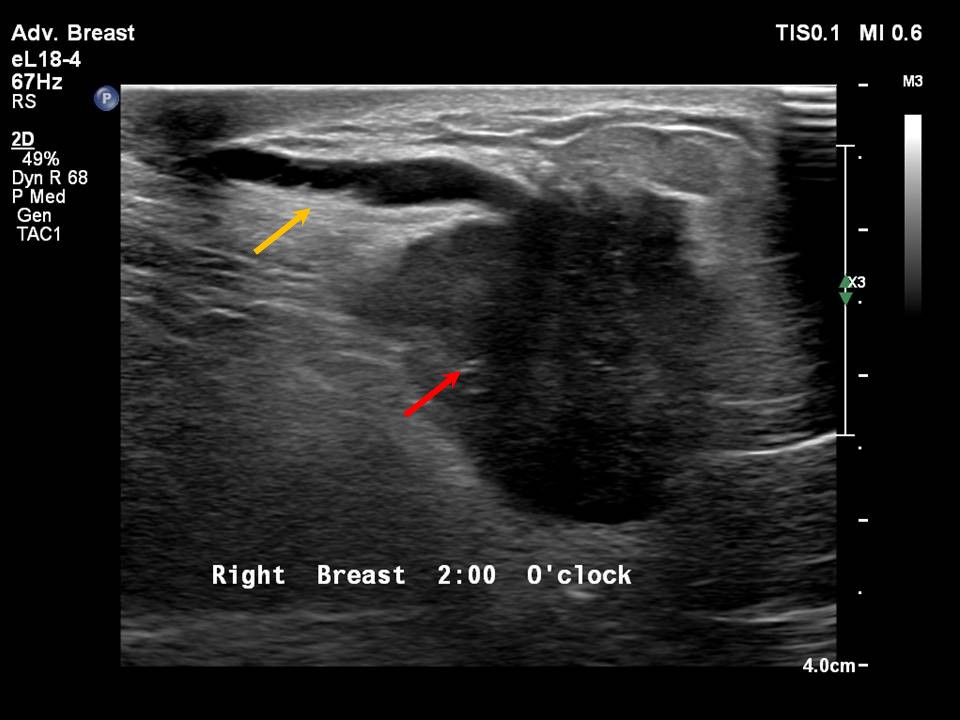
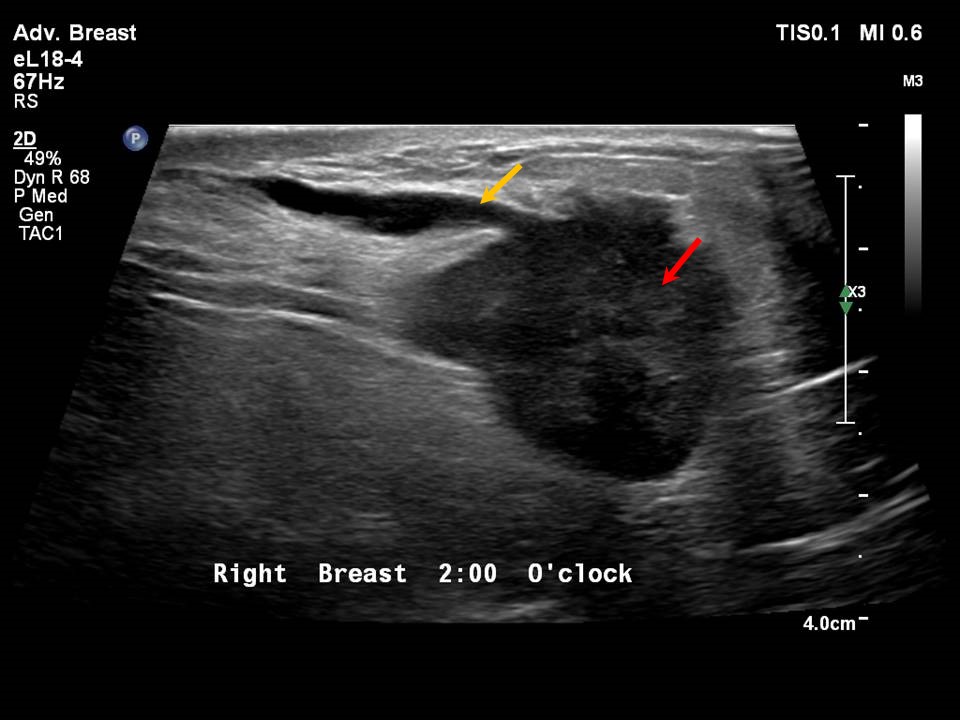
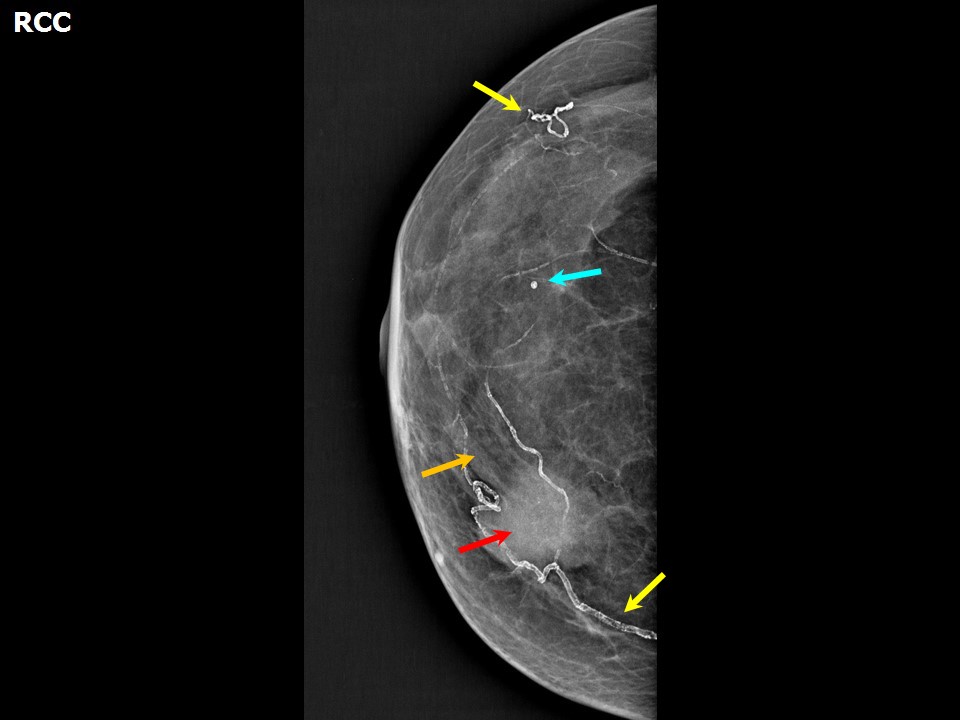
Physiological lactational changes Physiological lactational changes may be seen in both breasts as proliferation of the fatty and glandular tissue and duct dilatation with fine mobile echoes of the colostrum and milk product secretions in the ducts. The changes are variable in different women but are almost uniform and symmetrical in the two breasts of the same woman. Ultrasound is considered the method of choice during pregnancy and lactation; it has a sensitivity of 86.7% during pregnancy and 100.0% during lactation in symptomatic women. Ultrasound effectively assesses the breast anomalies without exposure to ionizing radiation. Breast infection or inflammation (mastitis) Ultrasound is the imaging modality of choice for the evaluation of women presenting with symptoms of breast infection and inflammation, in both puerperal and non-puerperal stages. Ultrasound reveals morphological changes caused by inflammation, such as altered echogenicity of the breast tissue, breast oedema, dilated ducts with thickened walls and echogenic intraductal debris, increased vascularity on colour Doppler, and reactive axillary nodes. These changes indicate pathological duct dilatation and are specific to the duct involved. Mammary duct ectasia Mammary duct ectasia is common in women aged 5060 years who are in the perimenopausal period. Normal breast ducts measure < 1.52 mm in diameter. In duct ectasia the ducts are > 2.53 mm in diameter with no solid intraductal lesion and no associated breast mass. The presenting symptoms are nipple discharge, nipple retraction, and breast pain or tenderness. The age-specific changes of chronic inflammatory and fibrotic changes in the involuting breasts lead to debris clogging the ducts, and this results in duct dilatation. Duct dilatation is not symmetrical in the two breasts of the same woman and is an evolving change seen in different ducts in both breasts through the transitional changes of involution. Breast neoplasm Duct changes may be seen as an associated feature of breast malignancy. The common appearances on breast ultrasound are dilated ducts seen along a mass that has the morphological features of malignancy. A mass lesion and a dilated duct from the nipple to the mass indicates the site of origin of the duct carcinoma along the ductal epithelium. These are diagnostic features and confirm a radiopathological diagnosis. A solitary duct or multiple dilated ducts with intraductal solid lesions are pathognomonic features of intraductal papilloma or papillary carcinoma. On ultrasound, this is seen as a solid non-mobile echogenic lesion along the duct wall, with a vascular stalk at the base of the lesion visible on colour Doppler .Subareolar dilated ducts with nippleareolar changes raise the possibility of Paget disease. On ultrasound, a dilated duct with mass lesion is seen in the areolar region. The presence of non-healing ulceration of the nippleareola region with or without nipple discharge helps to distinguish from infective aetiology. Biopsy of the non-healing ulcer will confirm the diagnosis. Echogenic intraductal foci merit further image-guided cytological workup to look for malignancy . |



Click on the pictures to magnify and display the legends
Click on this icon to display a case study
25 avenue Tony Garnier CS 90627 69366, LYON CEDEX 07 France - Tel: +33 (0)4 72 73 84 85
© IARC 2026 - Terms of use - Privacy Policy.
© IARC 2026 - Terms of use - Privacy Policy.