



Home / Training / Manuals / Atlas of breast cancer early detection / Cases
Atlas of breast cancer early detection
Filter by language: English / Русский
Go back to the list of case studies
.png) Click on the pictures to magnify and display the legends
Click on the pictures to magnify and display the legends
| Case number: | 056 |
| Age: | 58 |
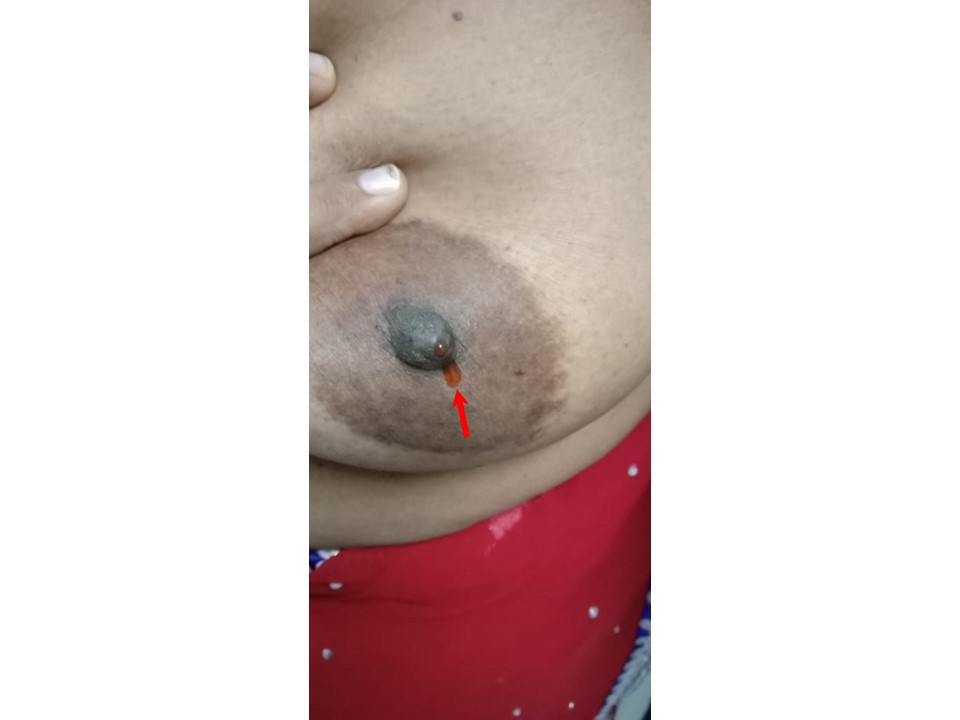
| Clinical presentation: | Postmenopausal woman with average risk of developing breast cancer presented with blood-stained nipple discharge from the left nipple. Examination did not reveal significant lumps in either breasts or axillae. |
 |
Mammography:
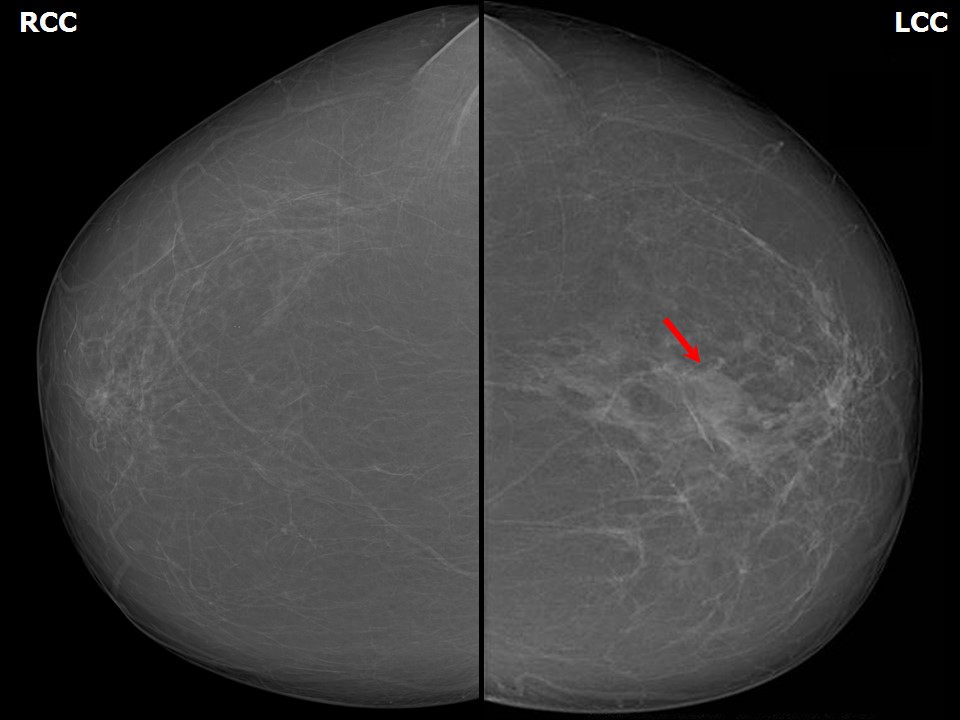 | 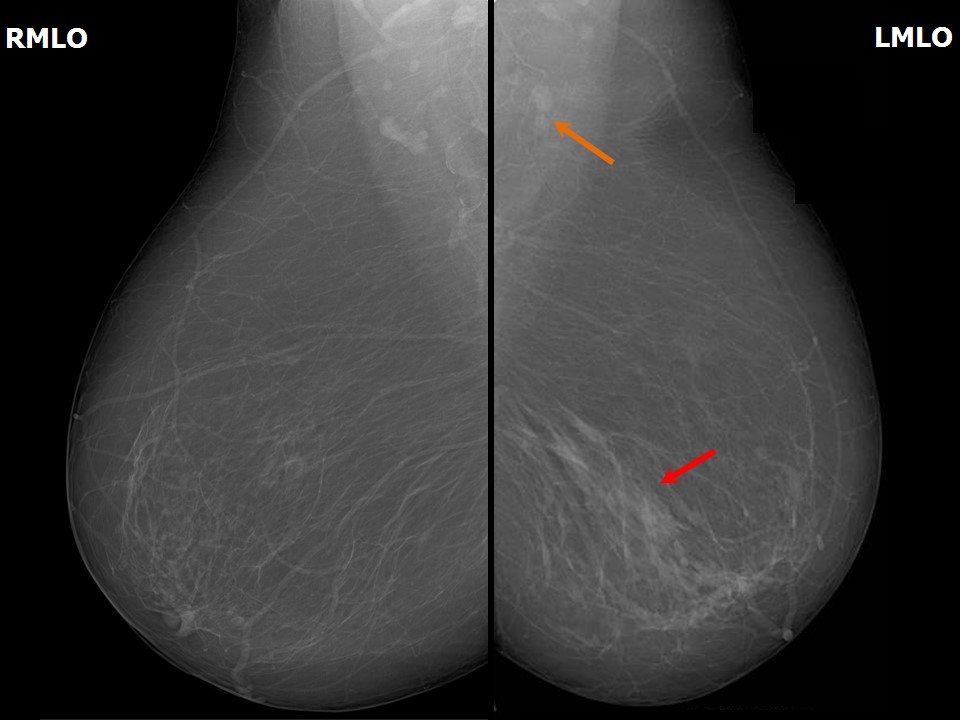 |
| Breast composition: | ACR category a (the breasts are almost entirely fatty) | Mammography features: |
| ‣ Location of the lesion: | Left breast, lower outer quadrant at 56 oclock, middle third |
| ‣ Mass: | |
| • Number: | Multiple small intraductal |
| • Size: | Not measurable |
| • Shape: | Indistinct |
| • Margins: | Obscured |
| • Density: | Equal |
| ‣ Calcifications: | |
| • Typically benign: | None |
| • Suspicious: | None |
| • Distribution: | None |
| ‣ Architectural distortion: | Present |
| ‣ Asymmetry: | Focal |
| ‣ Intramammary node: | None |
| ‣ Skin lesion: | None |
| ‣ Solitary dilated duct: | Multiple dilated ducts |
| ‣ Associated features: | Architectural distortion with linear opacities |
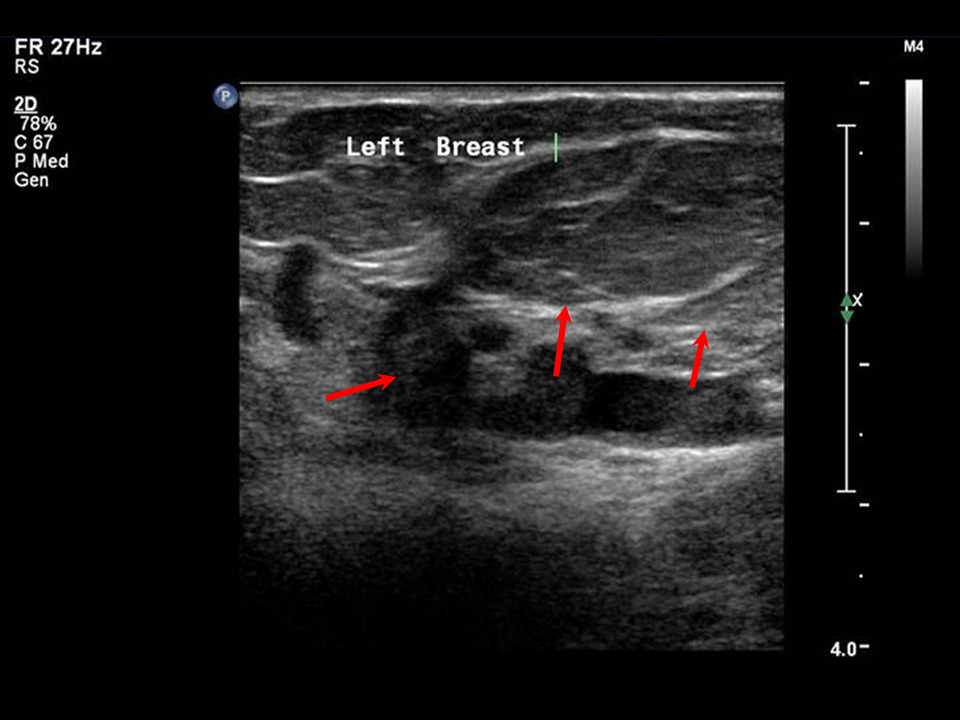
Ultrasound:
 |  |
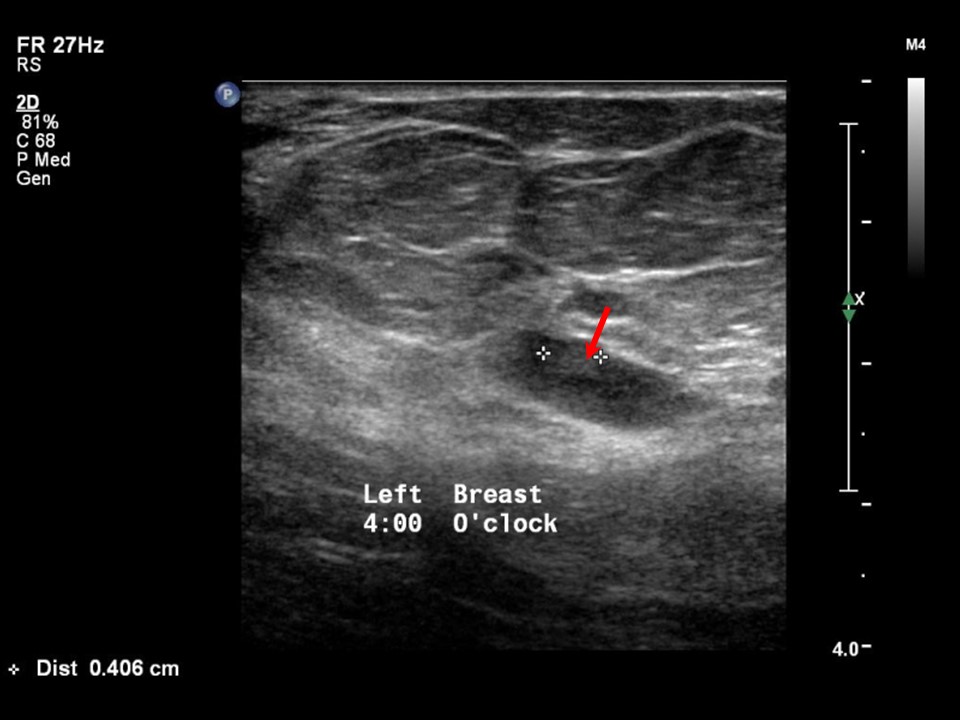 |
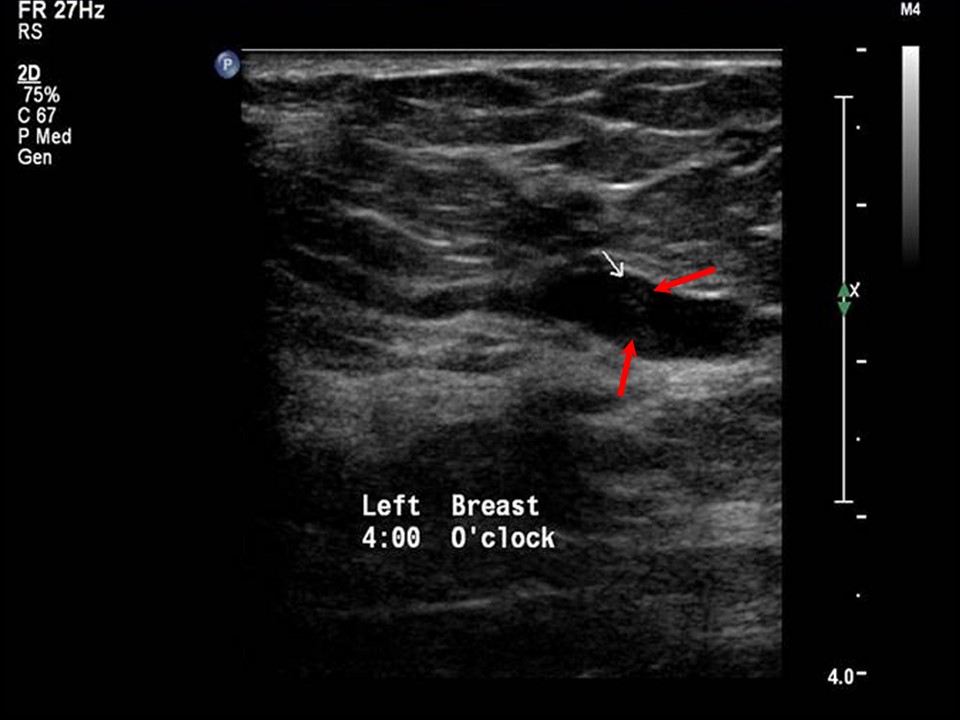
| Ultrasound features: Left breast, lower outer quadrant at 4 oclock | |
| ‣ Mass | |
| • Location: | Left breast, lower outer quadrant at 4 oclock |
| • Number: | Ultrasound transverse scan left breast shows multiple dilated ducts with intraductal lesions along the walls of the ducts |
| • Size: | Largest 0.4 cm in greatest dimension |
| • Shape: | Irregular |
| • Orientation: | Not parallel |
| • Margins: | Indistinct |
| • Echo pattern: | Hypoechoic |
| • Posterior features: | No posterior features |
| ‣ Calcifications: | None |
| ‣ Associated features: | Duct changes: ectatic duct with intraductal lesion along the walls |
| ‣ Special cases: | None |
BI-RADS:
BI-RADS Category: 4B (moderate suspicion of malignancy)Further assessment:
Further assessment advised: Further imaging with breast MRIMRI:
 |  |
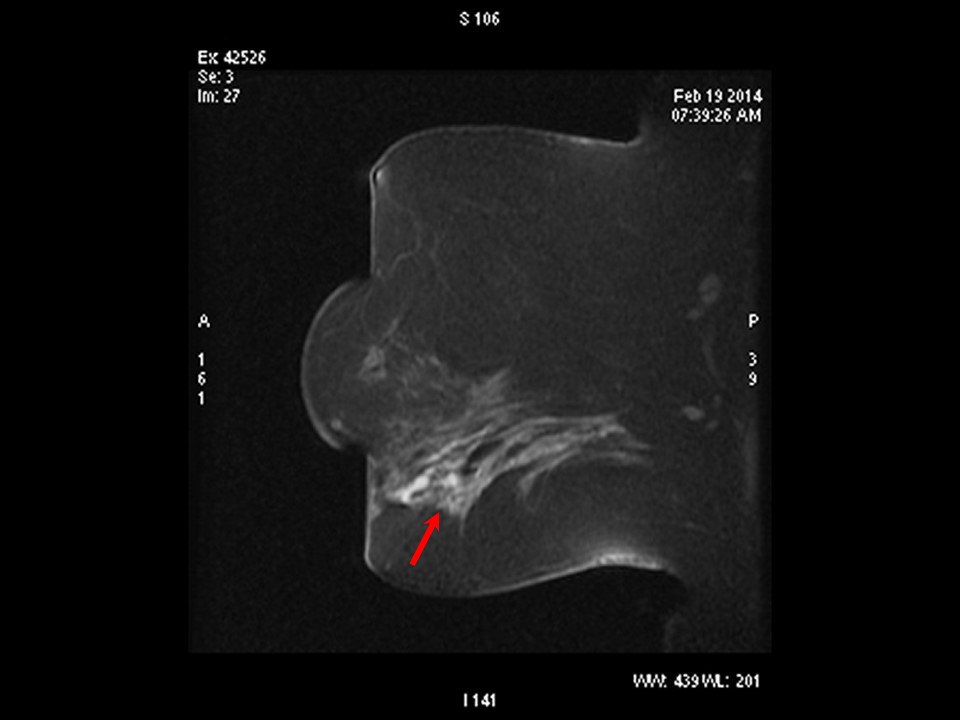 | 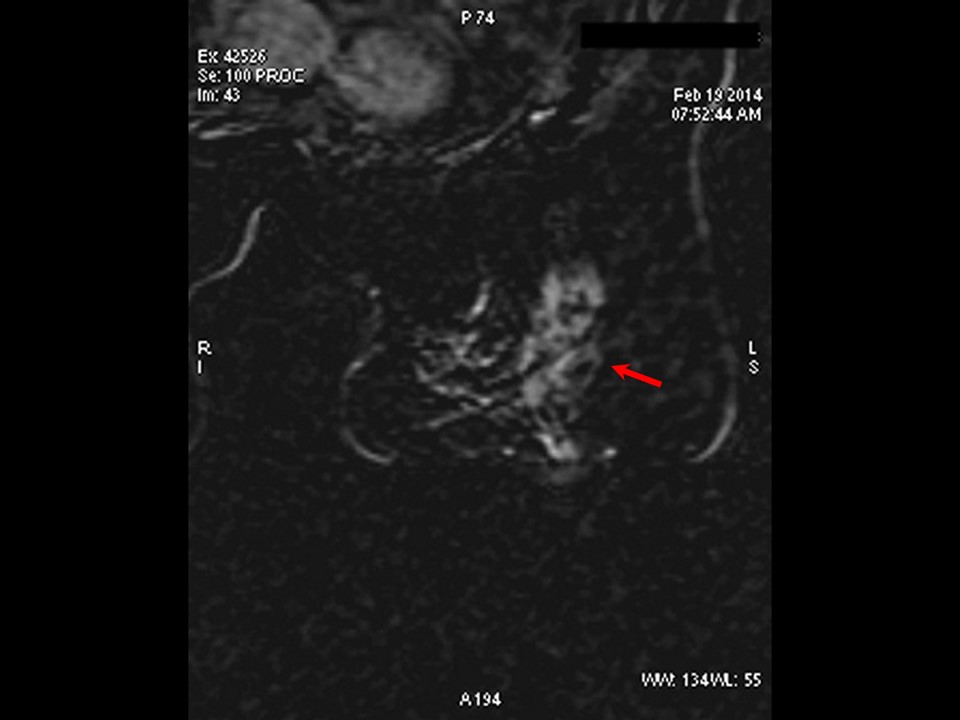 |
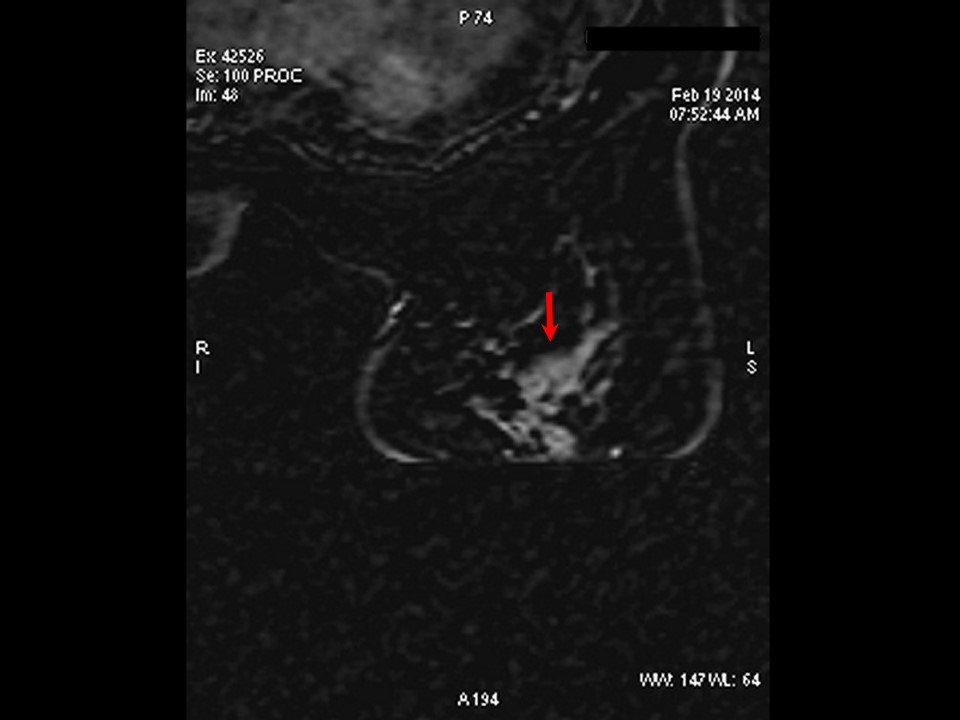 |
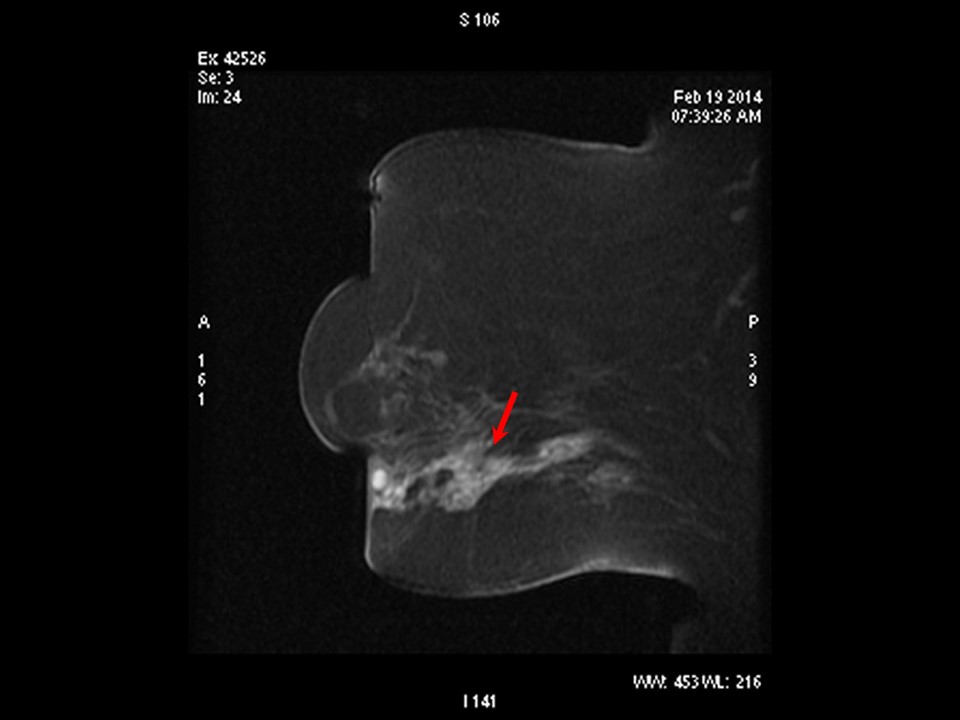
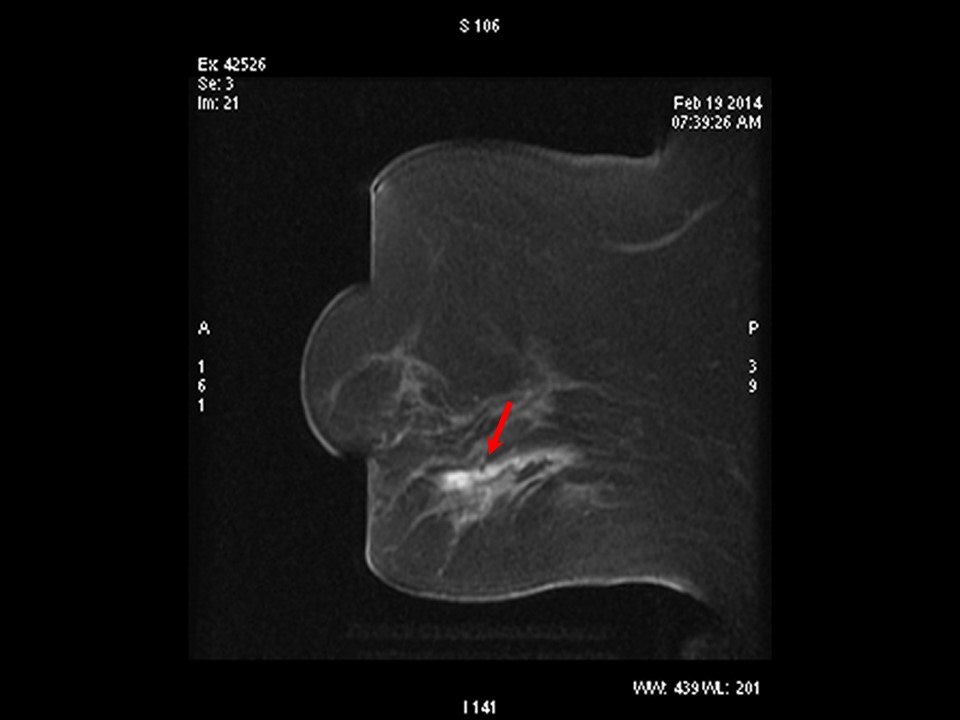
| MRI features: | ||
| ‣ MRI features: | Amount of fibroglandular tissue: ACR category a (the breasts are almost entirely fatty). Background parenchymal enhancement: Minimal (< 25%), symmetrical | |
| ‣ Location: | Left breast, lower quadrant | |
| ‣ Focus: | No | |
| ‣ Mass: | ||
| • Shape: | No | |
| • Margin: | No | |
| • Internal enhancement: | No | |
| • Kinetic curve: | No | |
| ‣ Non-mass enhancement: | ||
| • Distribution: | Intraductal and periductal non-mass-like enhancement in the inferior half at 58 oclock | |
| • Internal enhancement: | Heterogeneous | |
| ‣ Non-enhancing findings: | No | |
| ‣ Associated features: | Architectural distortion | |
| ‣ Axillary nodes: | No | |
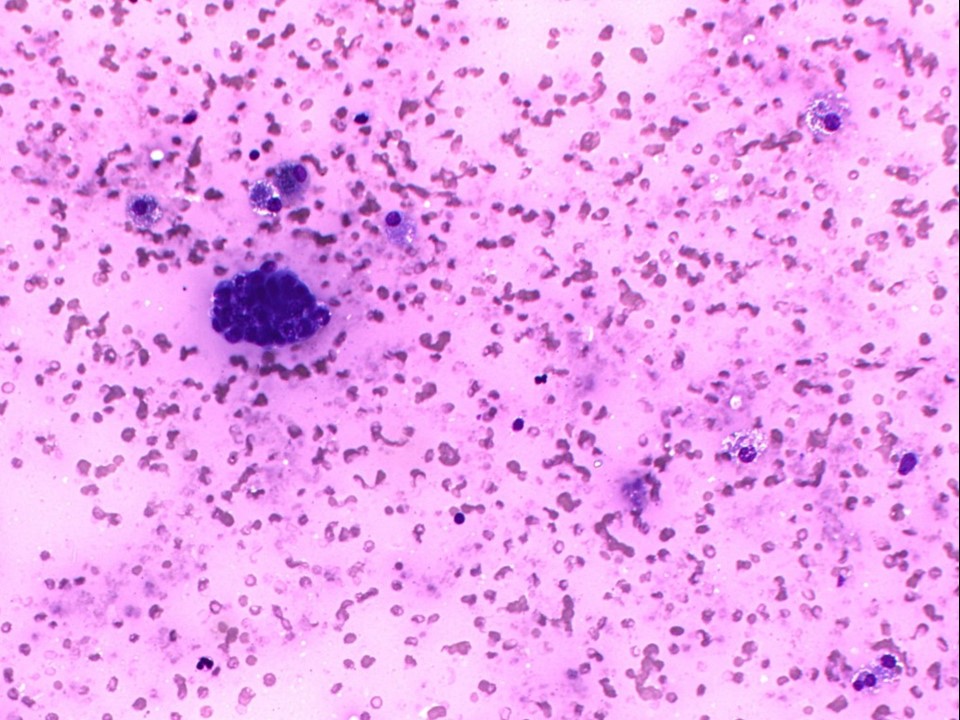
Cytology:
 |
| Cytology features: | |
| ‣ Type of sample: | Nipple discharge |
| ‣ Site of biopsy: | |
| • Laterality: | Left |
| • Quadrant: | |
| • Localization technique: | |
| • Nature of aspirate: | Brownish yellow discharge |
| ‣ Cytological description: | Smear from nipple discharge shows predominantly foamy macrophages and a few haemosiderin-laden macrophages. Occasional clusters of ductal epithelial cells are seen showing nuclear atypia |
| ‣ Reporting category: | Atypical, probably benign |
| ‣ Diagnosis: | Atypical, probably benign. Category 3 of IAC Yokohama System is atypical, probably benign |
| ‣ Comments: | None |
 |
| Cytology features: | |
| ‣ Type of sample: | FNAC |
| ‣ Site of biopsy: | |
| • Laterality: | Left |
| • Quadrant: | Lower half |
| • Localization technique: | Palpation |
| • Nature of aspirate: | whitish |
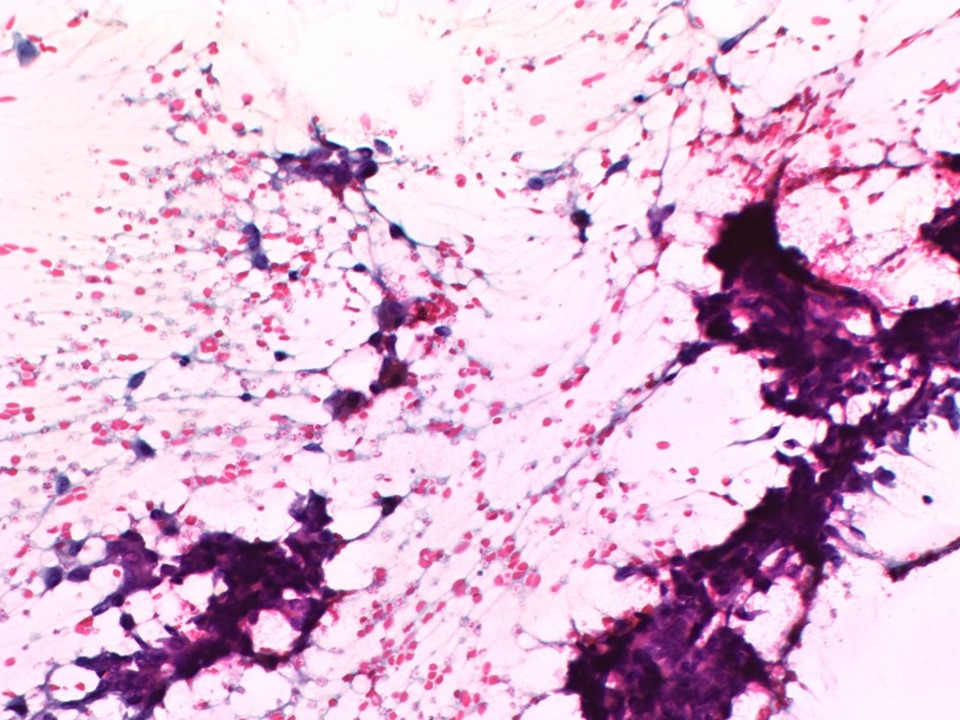
| ‣ Cytological description: | Smear shows many dyscohesive clusters and scattered solitary plasmacytoid cells with large pleomorphic nuclei and moderate cytoplasm. Background shows presence of RBCs and many macrophages; a few are haemosiderin laden. Many fibroadipose tissue fragments are also seen |
| ‣ Reporting category: | Suspicious, probably in situ or invasive carcinoma |
| ‣ Diagnosis: | Suspicious, probably in situ or invasive carcinoma |
| ‣ Comments: | None |
Histopathology:
MRM
 |  |
| Histopathology features: | |
| ‣ Specimen type: | MRM |
| ‣ Laterality: | Left |
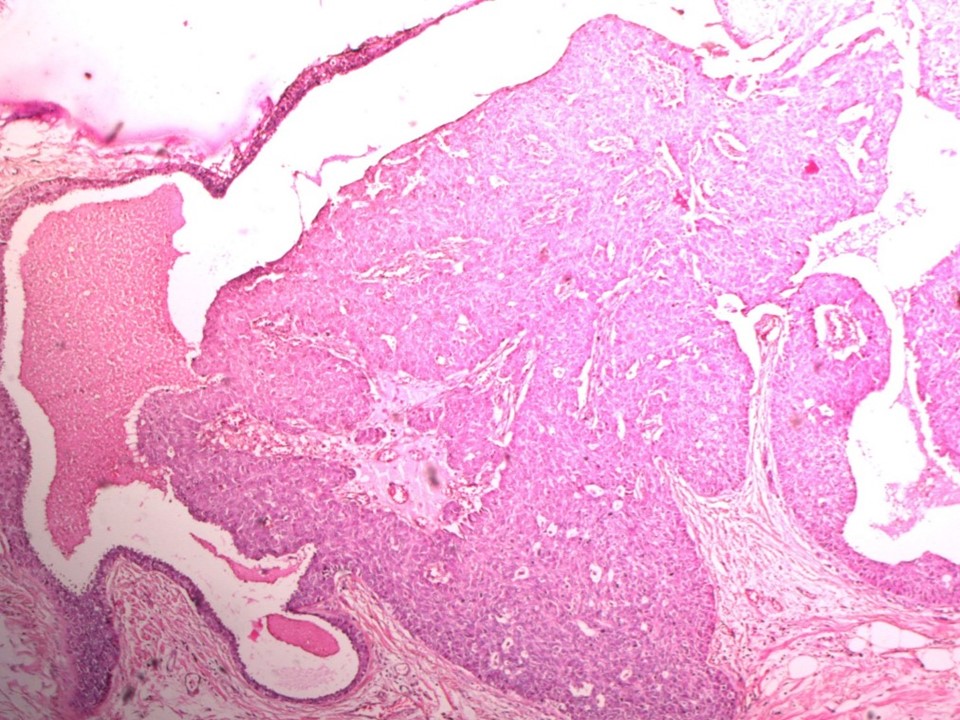
| ‣ Macroscopy: | On serial sectioning, a firm grey white area (7.8 × 3.0 × 2.5 cm) is seen in the central and lower quadrants. It is 3.0 cm from the skin and 1.5 cm from the base. The remaining breast tissue appears unremarkable |
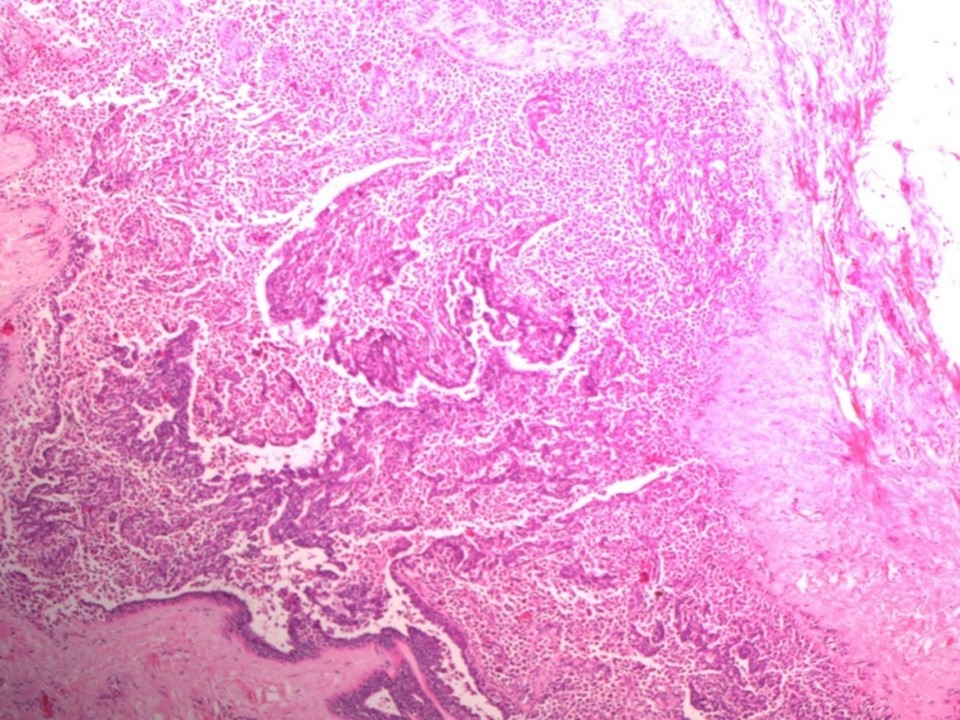
| ‣ Histological type: | Intraductal papillary carcinoma with invasive carcinoma |
| ‣ Histological grade: | Grade 2 (3 + 2 + 1 = 6) |
| ‣ Mitosis: | 3 |
| ‣ Maximum invasive tumour size: | 0.7 cm in greatest dimension |
| ‣ Lymph node status: | 0/15 |
| ‣ Peritumoural lymphovascular invasion: | Absent |
| ‣ DCIS/EIC: | DCIS of solid, micropapillary, papillary, and flat-type intermediate grade; EIC present with multiple foci of microinvasion |
| ‣ Margins: | Free of tumour, distance from nearest margin (i.e. base) 0.7 cm |
| ‣ Pathological stage: | pT1N0 |
| ‣ Biomarkers: | |
| ‣ Comments: | The intraductal papillary carcinoma involves several large ducts, a few of which are cystically dilated with papillary carcinoma within the duct. Multiple foci of microinvasion are seen |
Case summary:
| Postmenopausal woman presented with left breast blood-stained nipple discharge, diagnosed as multiple dilated ducts with intraductal solid lesions in the left breast, BI-RADS category 4B on imaging, as suspicious, probably in situ or invasive carcinoma, left breast on cytology, and as intraductal papillary carcinoma with invasive carcinoma on histopathology. |
Learning points:
|