



Home / Training / Manuals / Atlas of breast cancer early detection / Cases
Atlas of breast cancer early detection
Filter by language: English / Русский
Go back to the list of case studies
.png) Click on the pictures to magnify and display the legends
Click on the pictures to magnify and display the legends
| Case number: | 175 |
| Age: | 66 |
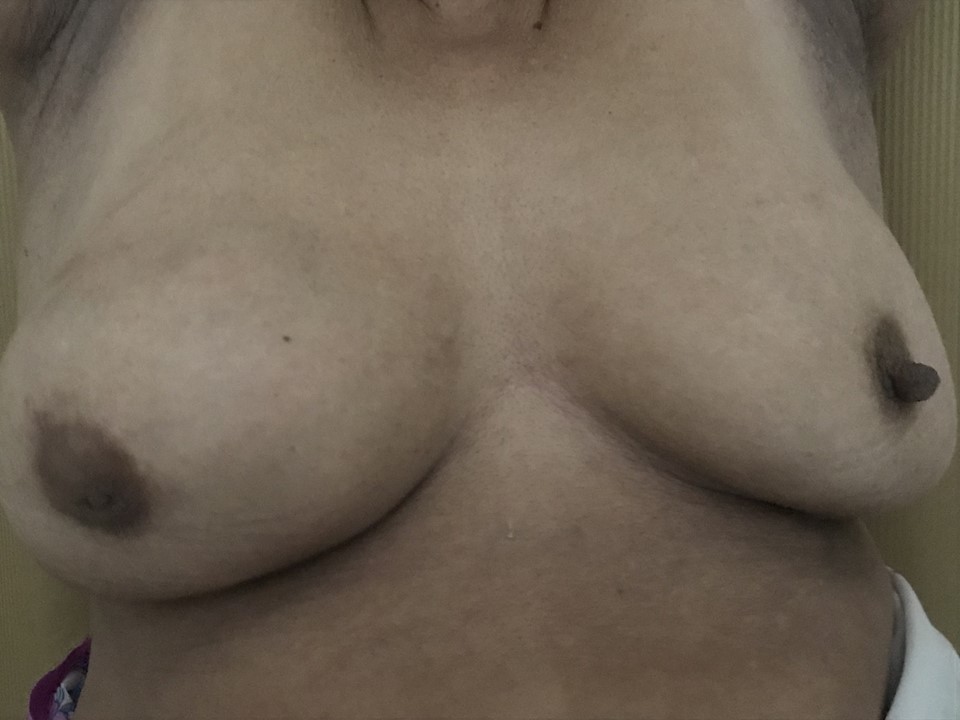
| Clinical presentation: | Postmenopausal woman with average risk of developing breast cancer presented with a right breast lump first noticed 4 years ago with progressive increase in size since then. On examination, a hard non-tender lump (5 × 5 cm) was palpable in the right breast below the nippleareolar complex. It was not fixed to the chest wall or skin and was fixed to the breast parenchyma. The right nipple was retracted. The left breast was unremarkable. A hard mobile lymph node (3 × 4 cm) was also palpable in the right axilla in a central group of axillary nodes. |
 |
Mammography:
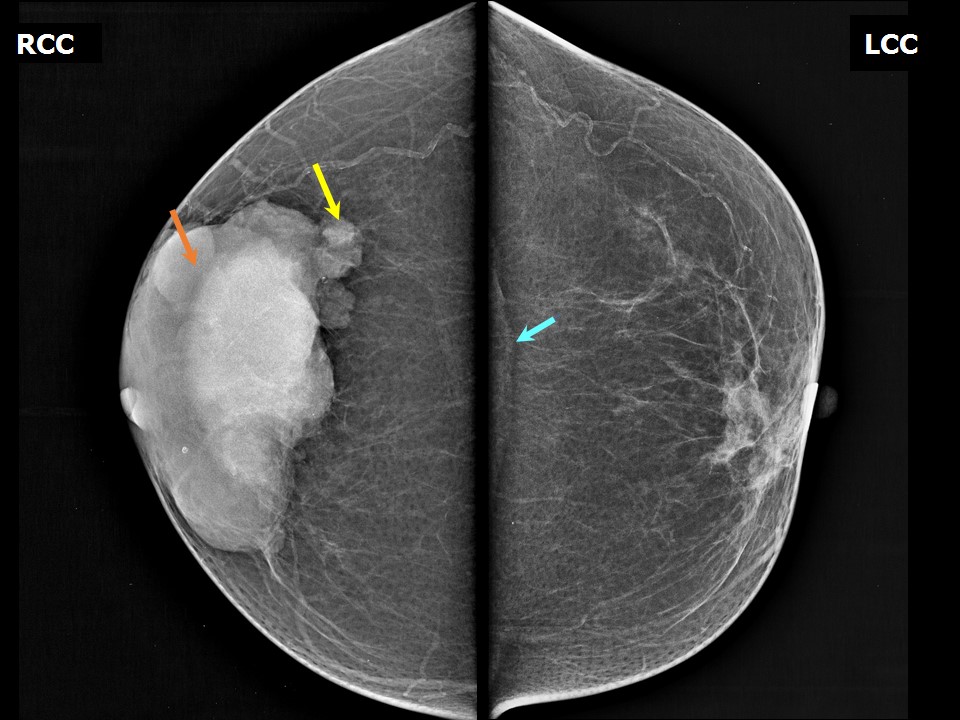 | 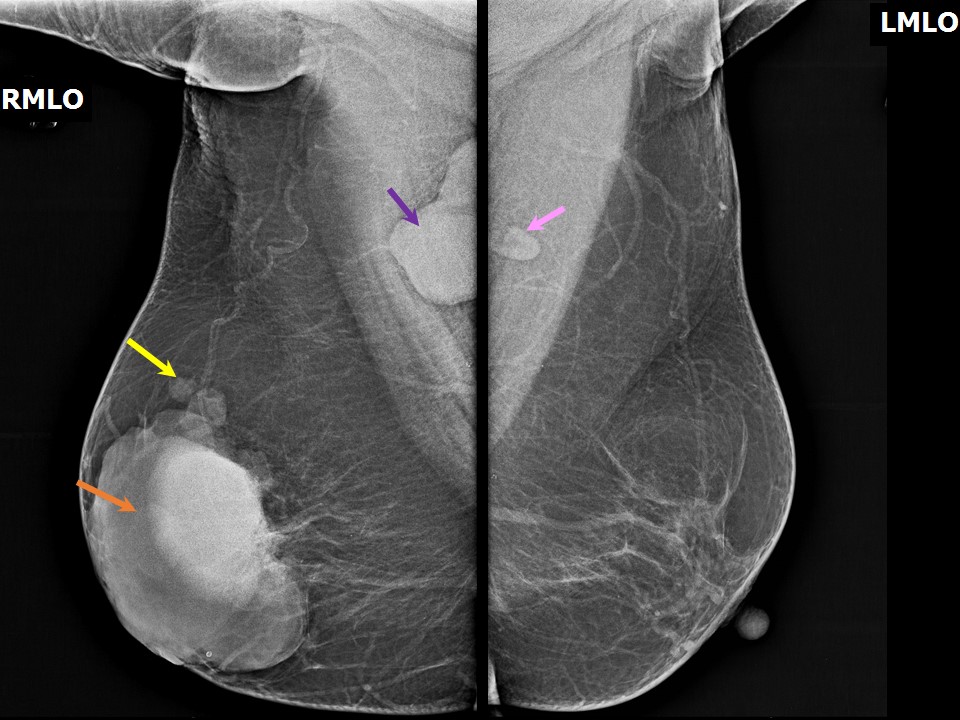 |
| Breast composition: | ACR category a (the breasts are almost entirely fatty) | Mammography features: |
| ‣ Location of the lesion: | Right breast, central portion of the breast, lower inner to upper outer quadrants at 610 oclock, anterior third |
| ‣ Mass: | |
| • Number: | 1 |
| • Size: | 10.5 × 6.5 cm |
| • Shape: | Irregular |
| • Margins: | Partly circumscribed and partly indistinct |
| • Density: | Yes, vascular in both breasts |
| ‣ Calcifications: | |
| • Typically benign: | None |
| • Suspicious: | None |
| • Distribution: | None |
| ‣ Architectural distortion: | None |
| ‣ Asymmetry: | None |
| ‣ Intramammary node: | None |
| ‣ Skin lesion: | None |
| ‣ Solitary dilated duct: | None |
| ‣ Associated features: | Nipple retraction and enlarged lymph nodal mass in right |
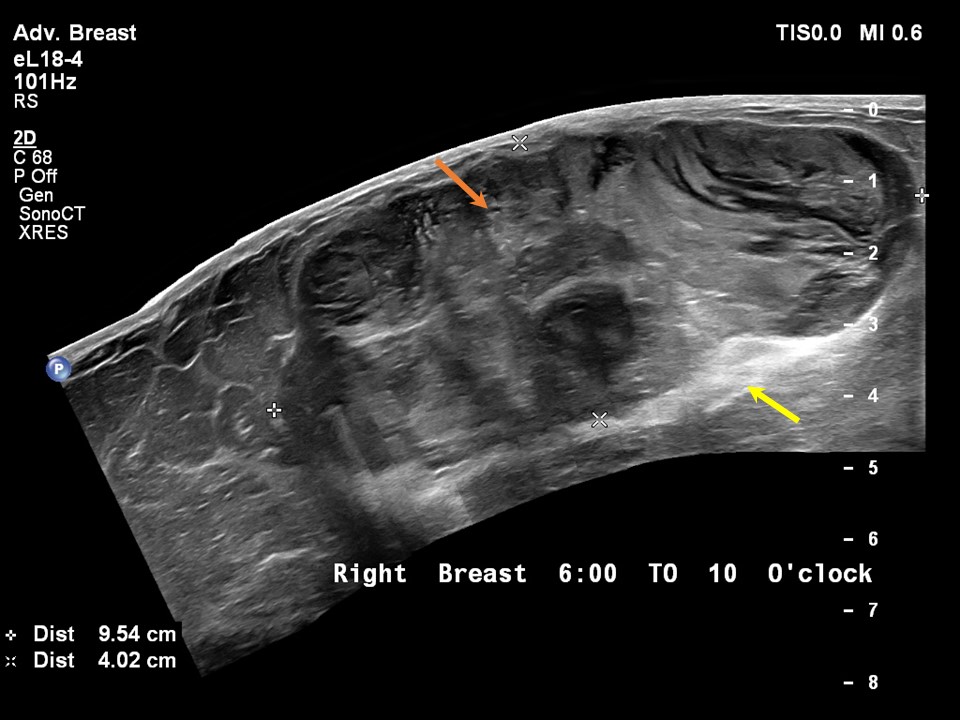
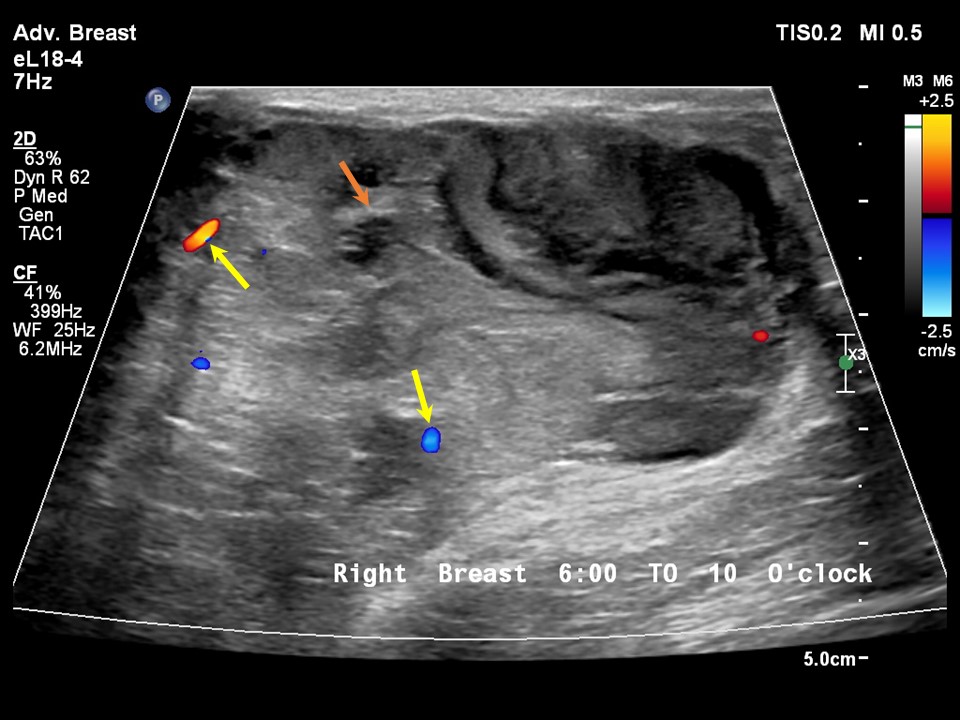
Ultrasound:
 |  |
 |
| Ultrasound features: Right breast, lower inner to upper outer quadrants at 510 oclock | |
| ‣ Mass | |
| • Location: | Right breast, lower inner to upper outer quadrants at 510 oclock |
| • Number: | 1 |
| • Size: | 9.5 × 4.0 cm |
| • Shape: | Oval |
| • Orientation: | Parallel |
| • Margins: | Circumscribed |
| • Echo pattern: | Heteroechoic with central anechoic component |
| • Posterior features: | Posterior shadowing |
| ‣ Calcifications: | None |
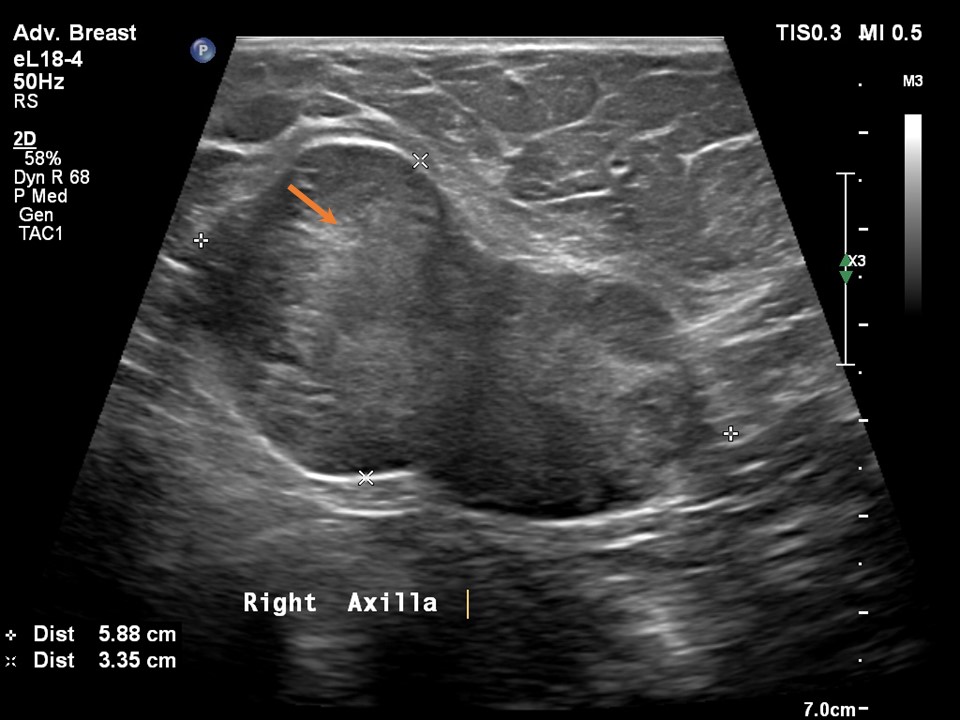
| ‣ Associated features: | Large right axillary nodal mass |
| ‣ Special cases: | None |
BI-RADS:
BI-RADS Category: 5 (highly suggestive of malignancy)Further assessment:
Further assessment advised: Referral for cytologyCytology:
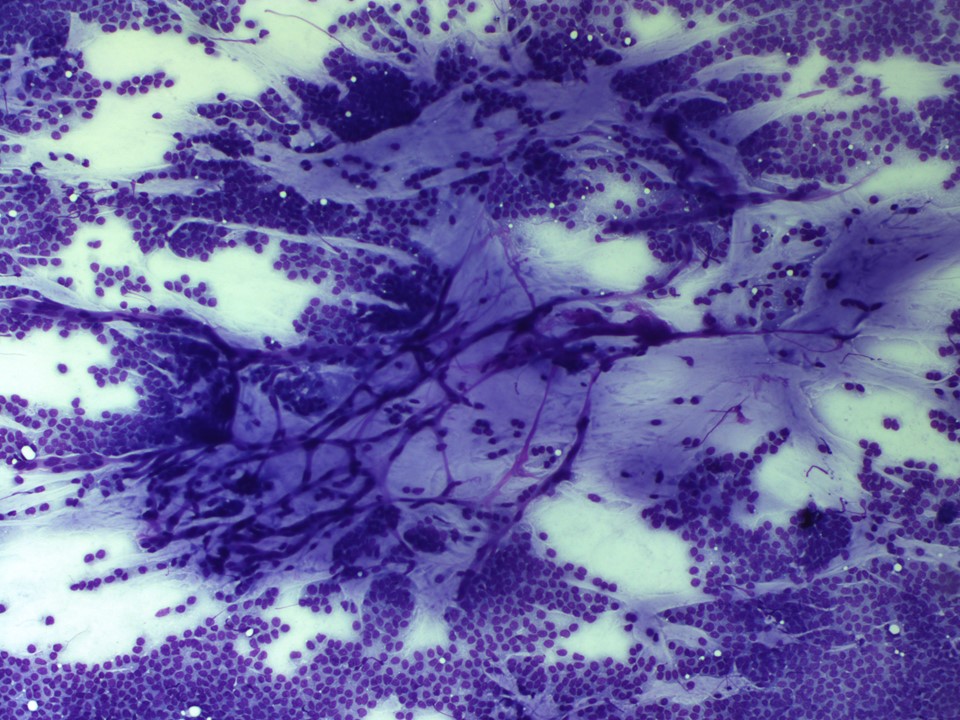 |  |
| Cytology features: | |
| ‣ Type of sample: | FNAC |
| ‣ Site of biopsy: | |
| • Laterality: | Left |
| • Quadrant: | Central |
| • Localization technique: | Palpation |
| • Nature of aspirate: | Whitish, mucinous material |
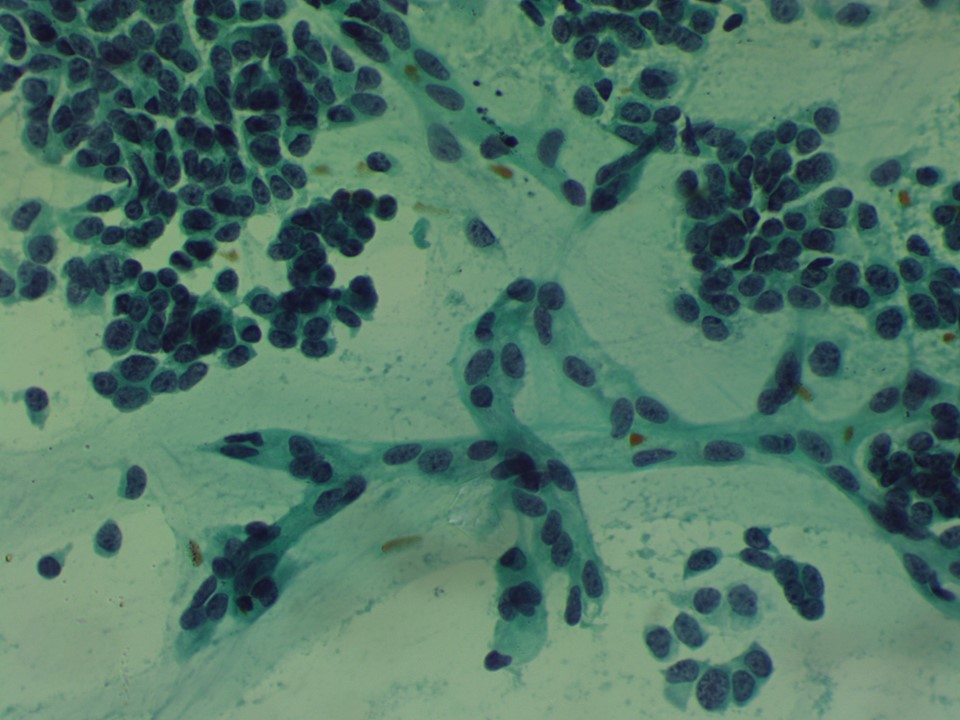
| ‣ Cytological description: | Smears show numerous tightly cohesive clusters dispersed in abundant mucinous material in the background. The malignant cells have low-grade, round, and regular nuclei |
| ‣ Reporting category: | Malignant |
| ‣ Diagnosis: | Carcinoma, likely mucinous |
| ‣ Comments: | None |
Histopathology:
Core needle biopsy
 | 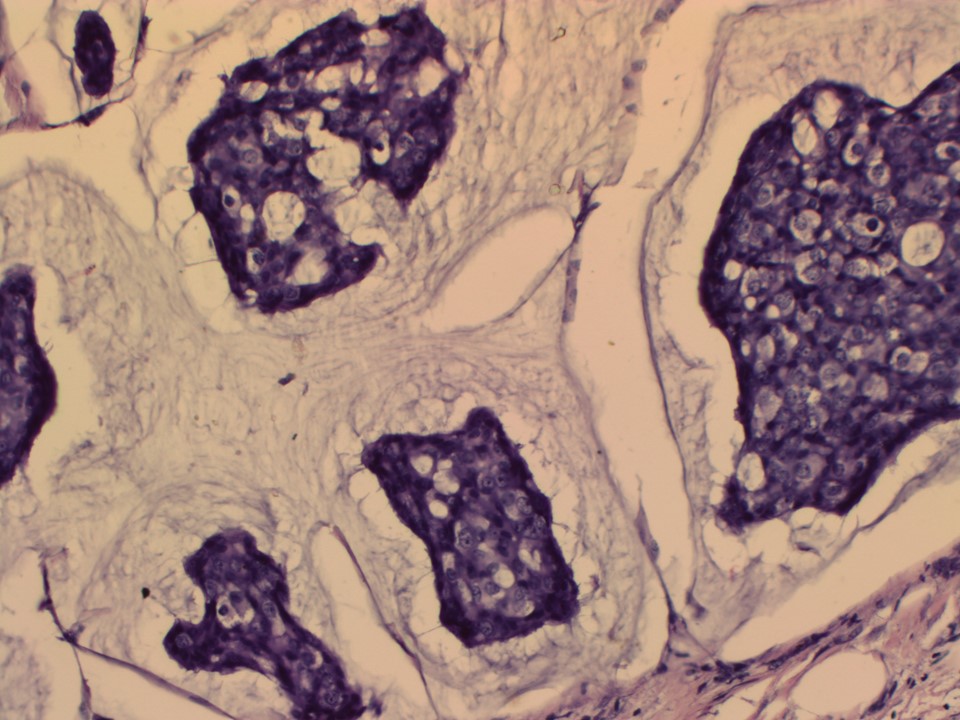 |
| Histopathology features: | |
| ‣ Specimen type: | Core needle biopsy |
| ‣ Laterality: | Right |
| ‣ Macroscopy: | Multiple linear greyish white tissue cores 313 mm in length |
| ‣ Histological type: | Invasion carcinoma with mucinous differentiation |
| ‣ Histological grade: | Grade 2 (3 + 2 + 1 = 6) |
| ‣ Mitosis: | 4 |
| ‣ Maximum invasive tumour size: | |
| ‣ Lymph node status: | |
| ‣ Peritumoural lymphovascular invasion: | |
| ‣ DCIS/EIC: | Not seen |
| ‣ Margins: | |
| ‣ Pathological stage: | |
| ‣ Biomarkers: | ER: Positive (100% of cells show nuclear staining with strong intensity. Allred score 8/8). PR: Positive (100% of cells show nuclear staining with strong intensity. Allred score 8/8). HER2: Negative |
| ‣ Comments: |
MRM
| Histopathology features: | |
| ‣ Specimen type: | MRM |
| ‣ Laterality: | Right |
| ‣ Macroscopy: | Specimen (18.0 × 16.0 × 6.5 cm) with skin flap (14.0 × 7.5 cm). Nipple and areola are retracted. On serial sectioning, a well-circumscribed tumour (9.5 × 6.3 × 5.2 cm) with gelatinous areas and intersecting fibrous septae is seen. It extends from the subareolar region in the central zone to the inner and outer quadrants. The tumour is 2.4 cm from the base and 0.3 cm from the skin. Adjacent breast tissue shows areas of fibrosis. The attached axillary fat tissue (9.0 × 6.0 × 4.5 cm) shows a well-circumscribed encapsulated nodule (5.5 × 3.0 × 2.5 cm). The mass shows gelatinous and cystic areas on the cut surface similar to breast tumour. Ten lymph nodes were dissected from the remaining tissue; the largest is 1.5 cm in diameter. Another specimen (3.0 × 2.5 × 0.4 cm) was labelled Level 3, interneural tissue. Four lymph nodes were dissected from this, the largest of which is 2.0 cm in diameter with a solid gelatinous cut surface |
| ‣ Histological type: | Mucinous carcinoma |
| ‣ Histological grade: | Grade 2 (3 + 2 + 1 = 6) |
| ‣ Mitosis: | 4 |
| ‣ Maximum invasive tumour size: | 9.5 cm in greatest dimension |
| ‣ Lymph node status: | 2/4 |
| ‣ Peritumoural lymphovascular invasion: | Absent |
| ‣ DCIS/EIC: | Not seen |
| ‣ Margins: | Free of tumour |
| ‣ Pathological stage: | pT3N3 |
| ‣ Biomarkers: | ER: 100% of tumour cells show intense nuclear positivity. Allred score 8/8. PR: 50% of tumour cells show moderate nuclear positivity. Allred score 6/8. HER2/neu: Negative |
| ‣ Comments: | The large nodule in axillary tissue shows metastatic tumour deposits of mucinous carcinoma with a thin rim of lymphoid tissue. The remaining adjacent 10 lymph nodes show reactive lymphoid hyperplasia, free of tumour. Two out of four lymph nodes from level 3 show metastasis of mucinous carcinoma |
Case summary:
| Postmenopausal woman presented with a lump in the right breast. Diagnosed as right breast carcinoma with large right axilla nodal mass, BI-RADS 5 on imaging, as mucinous carcinoma on cytology, and as mucinous carcinoma, pT3N3 on histopathology. |
Learning points:
|