



Home / Training / Manuals / Atlas of breast cancer early detection / Cases
Atlas of breast cancer early detection
Filter by language: English / Русский
Go back to the list of case studies
.png) Click on the pictures to magnify and display the legends
Click on the pictures to magnify and display the legends
| Case number: | 123 |
| Age: | 69 |
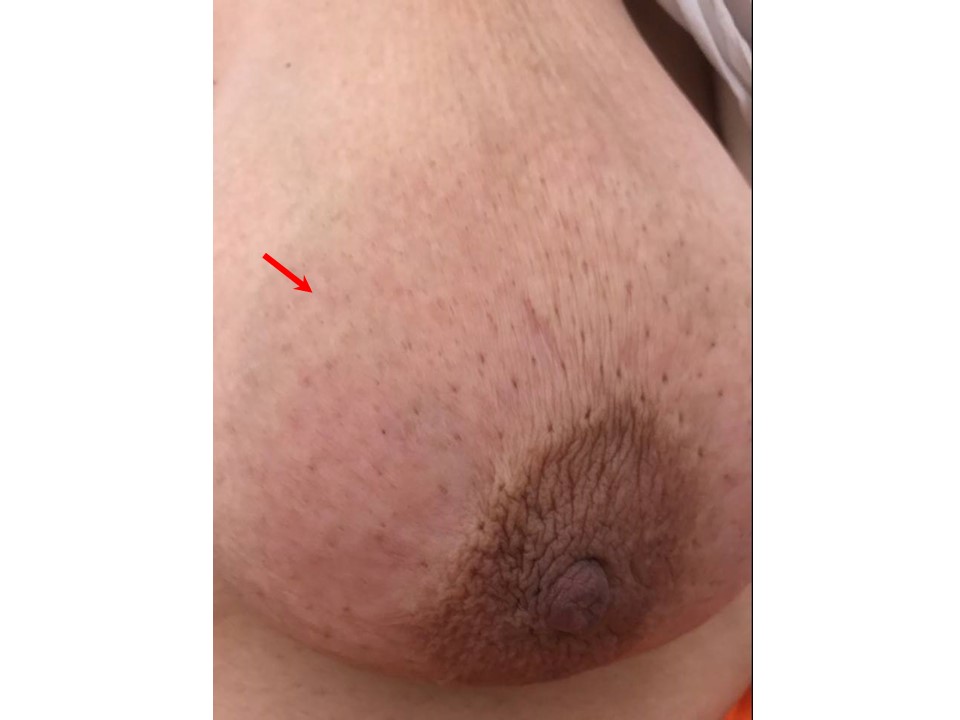
| Clinical presentation: | Postmenopausal woman with average risk of developing breast cancer presented with redness of skin over the left breast upper quadrant. Examination revealed redness of the skin around nippleareolar complex in the upper half of the left breast and an enlarged and palpable left axillary nodal mass. |
 |
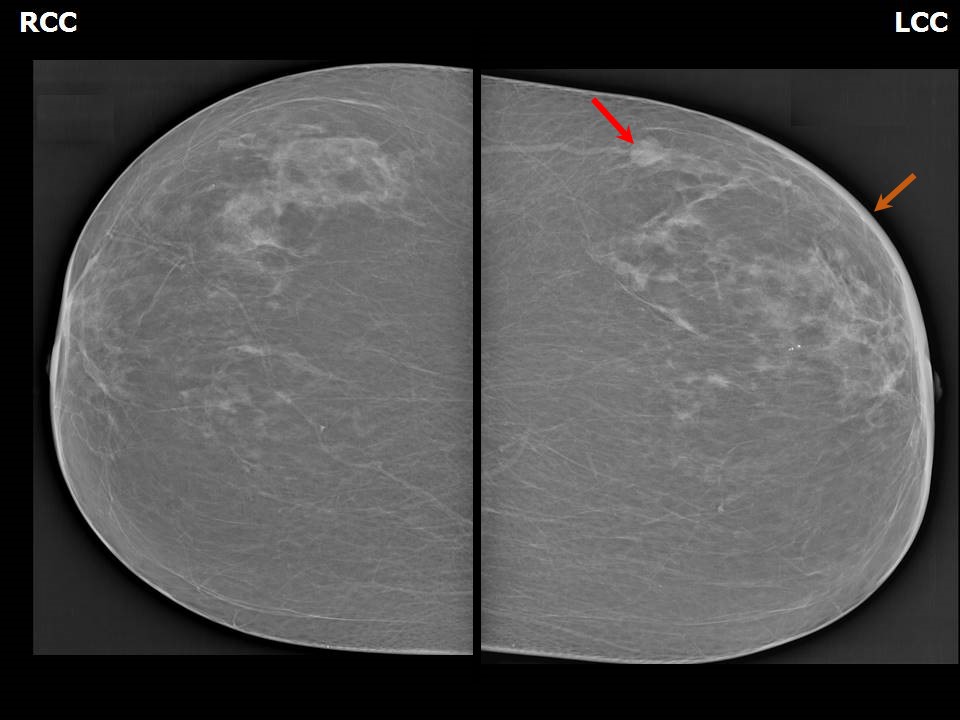
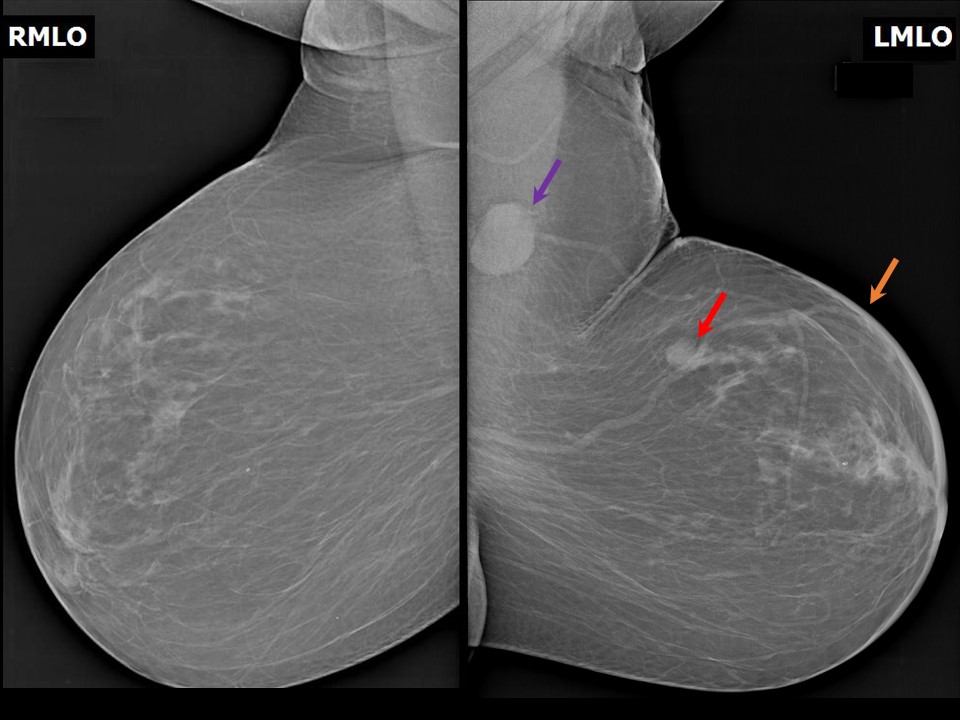
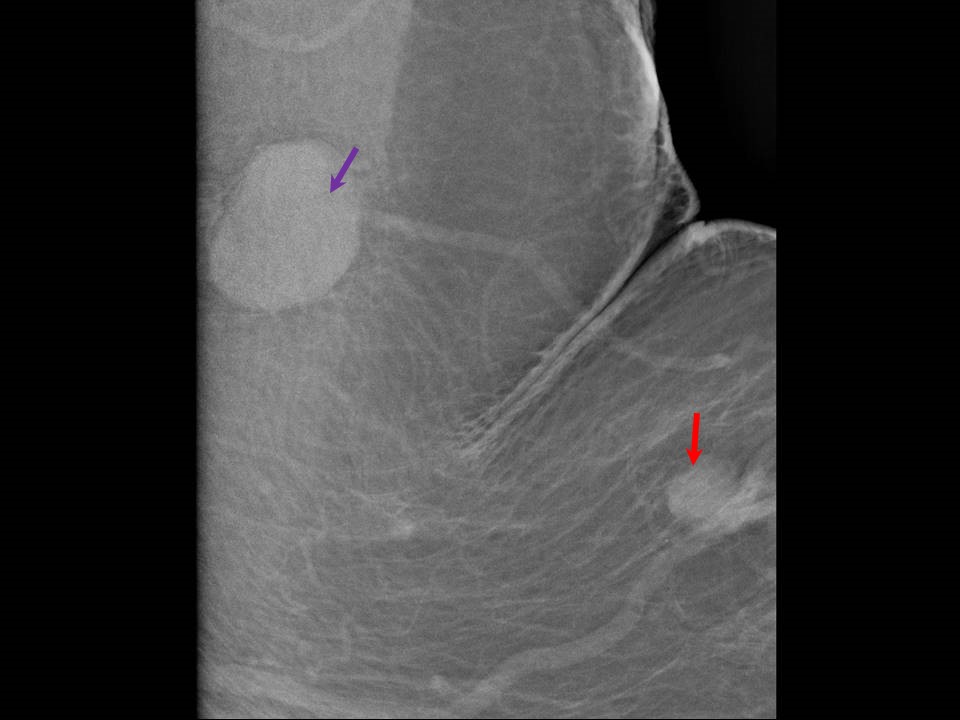
Mammography:
 |  |
 |
| Breast composition: | ACR category a (the breasts are almost entirely fatty) | Mammography features: |
| ‣ Location of the lesion: | Left breast, upper outer quadrant at 3 oclock, middle and posterior thirds |
| ‣ Mass: | |
| • Number: | 1 |
| • Size: | 1.5 × 1.2 cm |
| • Shape: | Oval |
| • Margins: | Indistinct |
| • Density: | Equal |
| ‣ Calcifications: | |
| • Typically benign: | None |
| • Suspicious: | None |
| • Distribution: | None |
| ‣ Architectural distortion: | None |
| ‣ Asymmetry: | None |
| ‣ Intramammary node: | None |
| ‣ Skin lesion: | None |
| ‣ Solitary dilated duct: | None |
| ‣ Associated features: | Enlarged high-density axillary node (3.3 × 2.7 cm) with loss of fatty hilum. Skin thickening in outer quadrant and areolar region of left breast |
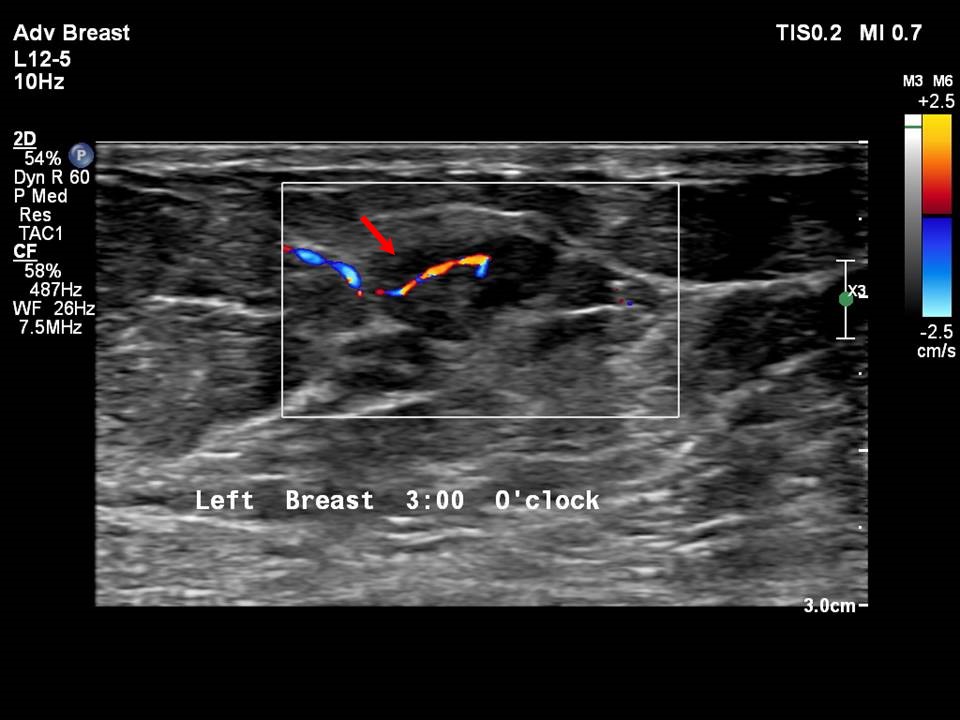
Ultrasound:
 |  |
 |
| Ultrasound features: Left breast, upper outer quadrant at 23 oclock | |
| ‣ Mass | |
| • Location: | Left breast, upper outer quadrant at 23 oclock |
| • Number: | 1 |
| • Size: | 1.3 × 1.0 cm |
| • Shape: | Irregular |
| • Orientation: | Parallel |
| • Margins: | Angular |
| • Echo pattern: | Hypoechoic |
| • Posterior features: | No posterior features |
| ‣ Calcifications: | None |
| ‣ Associated features: | Internal vascularity, skin thickening, and axillary lymphadenopathy (4.0 × 2.0 cm) with loss of fatty hilum |
| ‣ Special cases: | None |
BI-RADS:
BI-RADS Category: 5 (highly suggestive of malignancy)Further assessment:
Further assessment advised: Referral for cytologyCytology:
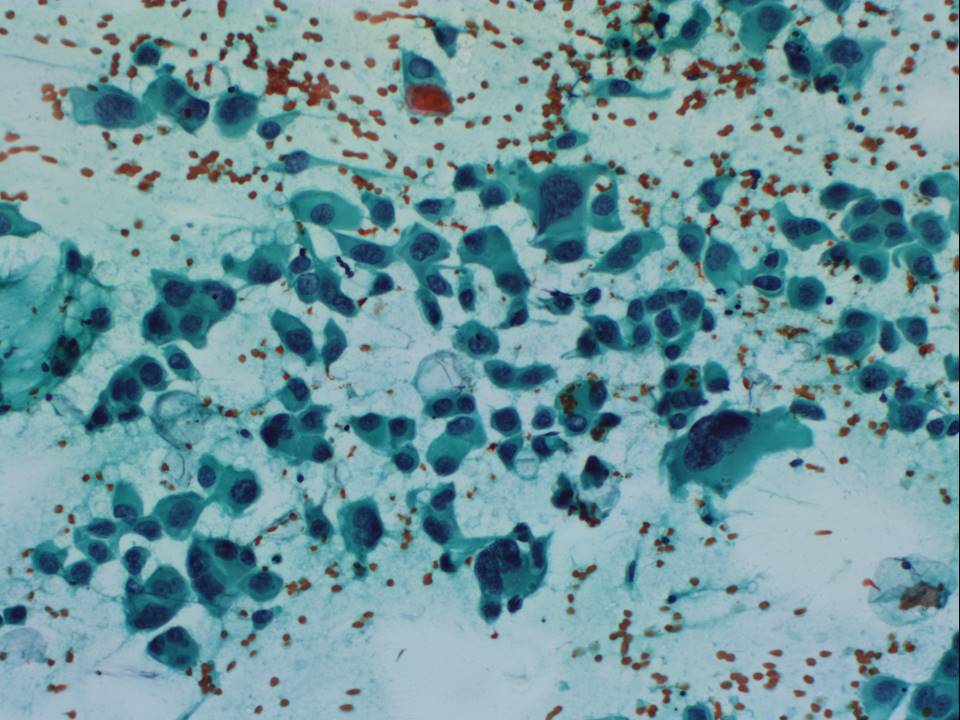 | 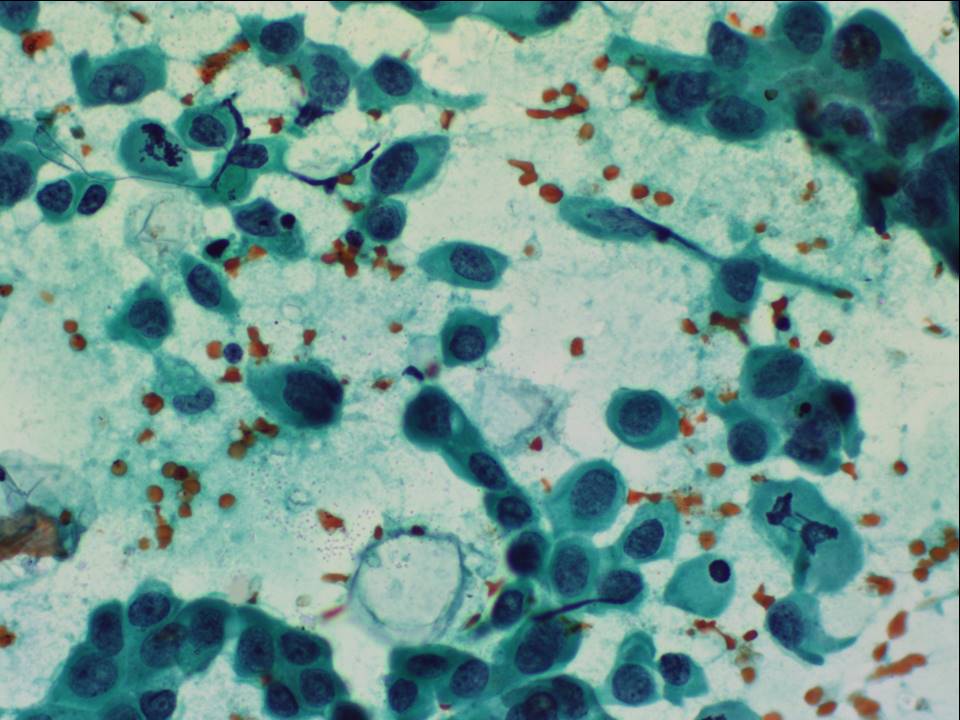 |
| Cytology features: | |
| ‣ Type of sample: | FNAC |
| ‣ Site of biopsy: | |
| • Laterality: | Left |
| • Quadrant: | Upper |
| • Localization technique: | Palpation |
| • Nature of aspirate: | whitish |
| ‣ Cytological description: | Smears are cellular and reveal many dyscohesive clusters and many dispersed large malignant cells. These cells have moderate cytoplasm and large hyperchromatic and pleomorphic nuclei with irregular nuclear margins and the presence of prominent nucleoli in many cells. Multinucleated tumour giant cells and mitotic figures are noted |
| ‣ Reporting category: | Malignant |
| ‣ Diagnosis: | Breast carcinoma high grade |
| ‣ Comments: | None |
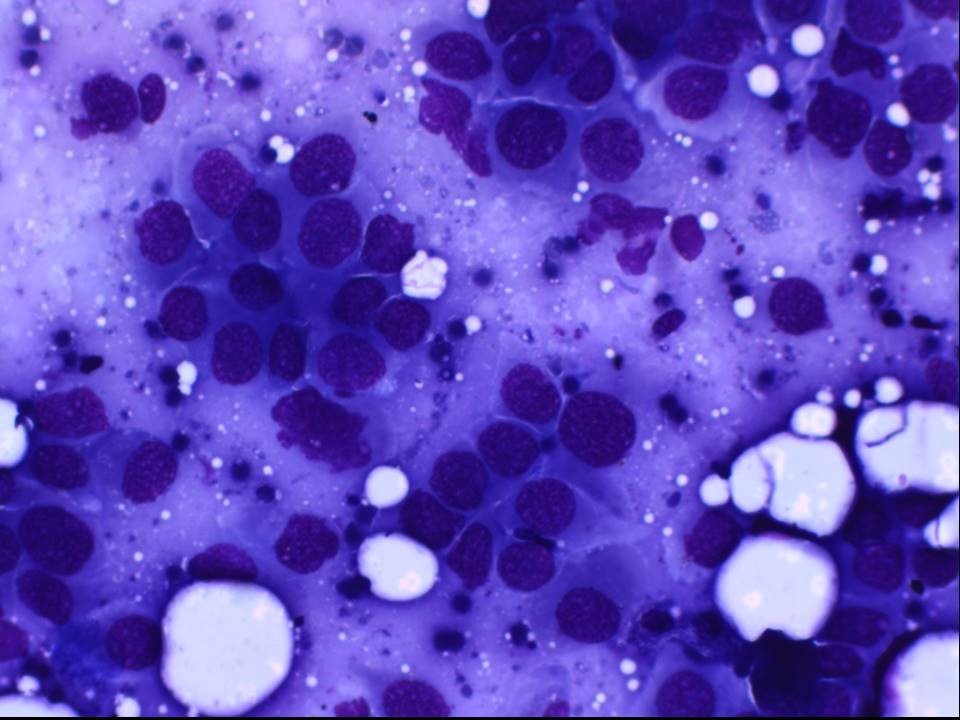 |
| Cytology features: | |
| ‣ Type of sample: | FNAC |
| ‣ Site of biopsy: | |
| • Laterality: | Left |
| • Quadrant: | Large axillary lump |
| • Localization technique: | Palpation |
| • Nature of aspirate: | Whitish |
| ‣ Cytological description: | Smears reveal large malignant cells in clusters and dispersed cells with morphology similar to that seen in the breast aspirate. Lymphoid cells are seen around the tumour cells and in the background |
| ‣ Reporting category: | Malignant |
| ‣ Diagnosis: | Nodal metastasis of breast carcinoma |
| ‣ Comments: | None |
Histopathology:
Breast-conserving surgery
 |  |
 |
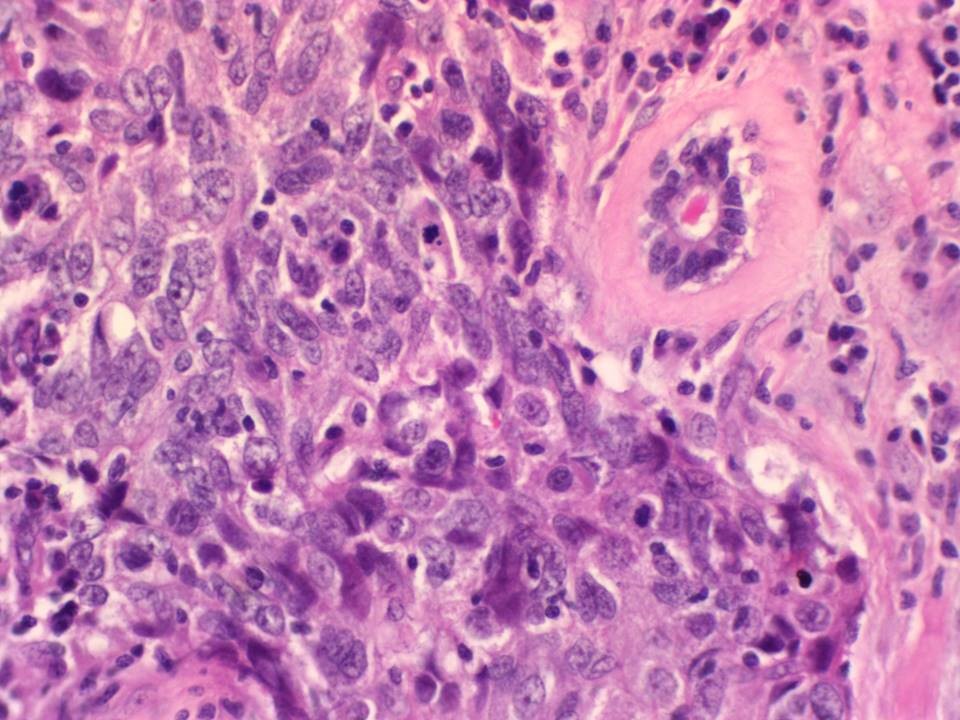
| Histopathology features: | |
| ‣ Specimen type: | Breast-conserving surgery |
| ‣ Laterality: | Left |
| ‣ Macroscopy: | Lumpectomy specimen (10.5 × 7.4 × 5.2 cm) oriented with long suture laterally and short suture superiorly and skin flap (4.0 × 0.2 cm). On serial sectioning, a hard white tumour (2.5 × 2.5 × 2.0 cm) is identified. It is located 0.5 cm from the anterior margin, 1.0 cm from the posterior margin, 1.0 cm from the superior margin, 2.0 cm from the inferior margin, 2.5 cm from the medial margin, and 5.0 cm from the lateral margin. Also identified is a firm white lesion (0.5 × 0.5 × 0.5 cm) that is 0.3 cm from the superior cut margin. It is 4.0 cm from the tumour |
| ‣ Histological type: | Invasive breast carcinoma of no special type |
| ‣ Histological grade: | Grade 3 (3 + 3 + 2 = 8) |
| ‣ Mitosis: | 15 |
| ‣ Maximum invasive tumour size: | 2.5 cm in greatest dimension |
| ‣ Lymph node status: | 9/23, with perinodal extension |
| ‣ Peritumoural lymphovascular invasion: | Absent |
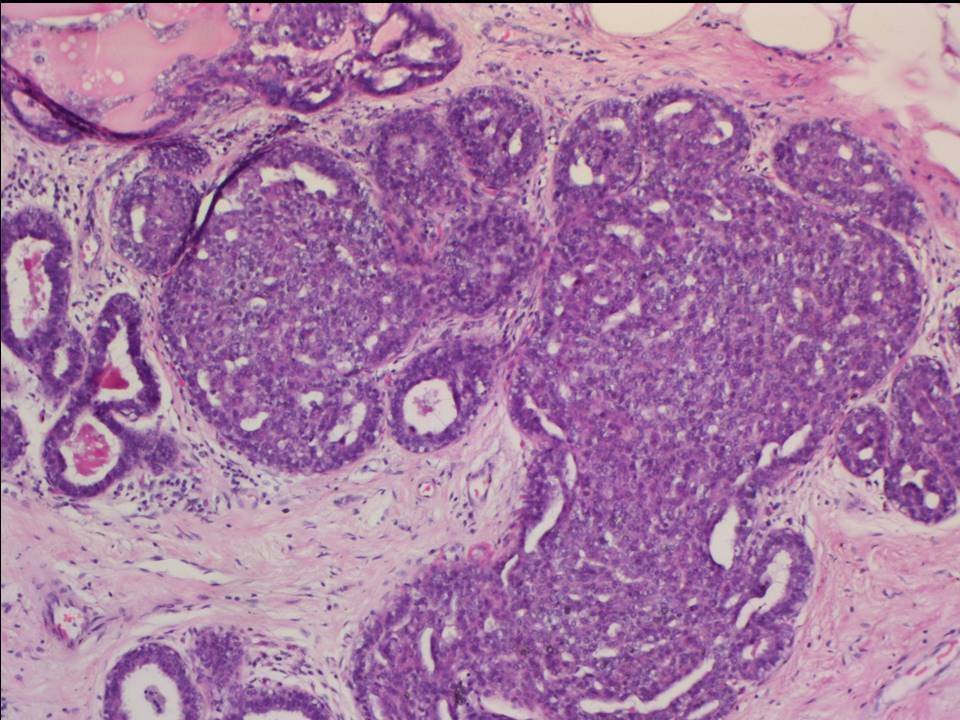
| ‣ DCIS/EIC: | DCIS identified, high nuclear grade with dystrophic calcification; EIC absent |
| ‣ Margins: | Free of tumour |
| ‣ Pathological stage: | pT2N2 |
| ‣ Biomarkers: | ER positive, PR positive, and HER2 positive (score 3+) |
| ‣ Comments: | The separate firm white lesion (0.5 × 0.5 × 0.5 cm) 4 cm away from the tumour shows features of UDH |
Case summary:
| Postmenopausal woman presented with redness of skin over the left breast upper quadrant and an enlarged palpable left axillary nodal mass. Diagnosed as left breast carcinoma with left axillary large node of altered morphology, BI-RADS 5 on imaging, as left breast carcinoma and axillary metastasis on cytology, and as invasive breast carcinoma of no special type, pT2N2 on histopathology. |
Learning points:
|