



Home / Training / Manuals / Atlas of breast cancer early detection / Cases
Atlas of breast cancer early detection
Filter by language: English / Русский
Go back to the list of case studies
.png) Click on the pictures to magnify and display the legends
Click on the pictures to magnify and display the legends
BI-RADS Category (2002): 2 (benign)
BI-RADS Category (2010): 5 (highly suggestive of malignancy)
| Case number: | 104 |
| Age: | 61 |
| Clinical presentation: | Postmenopausal woman with increased risk of developing breast cancer because of family history of breast cancer presented with nipple discharge. Examination revealed a small area of irregular thickening in the upper quadrant of the left breast. |
Mammography:
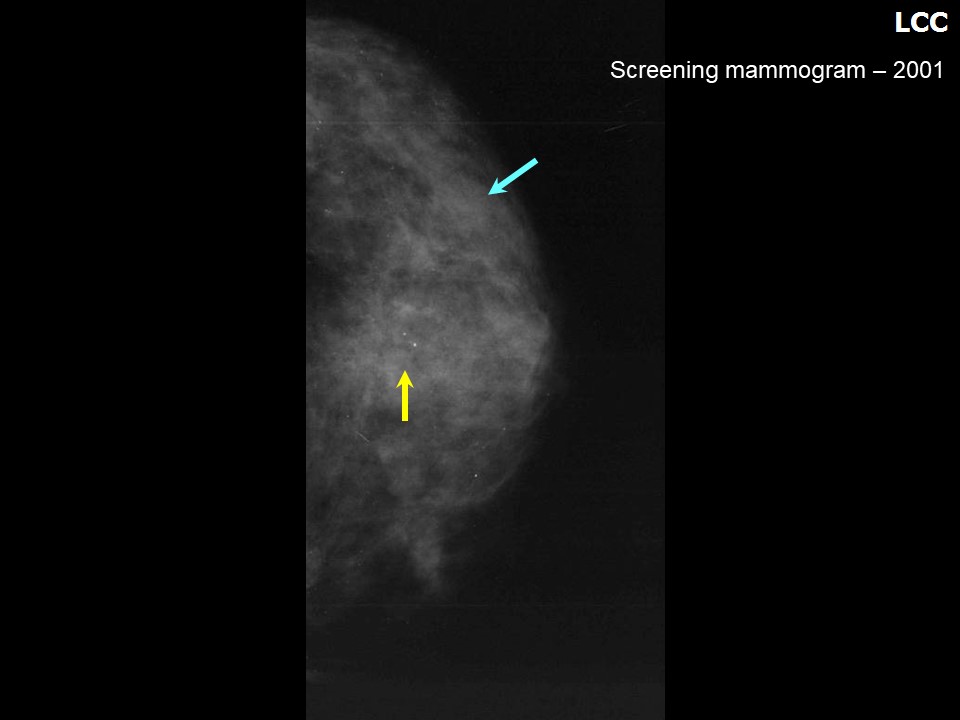 | 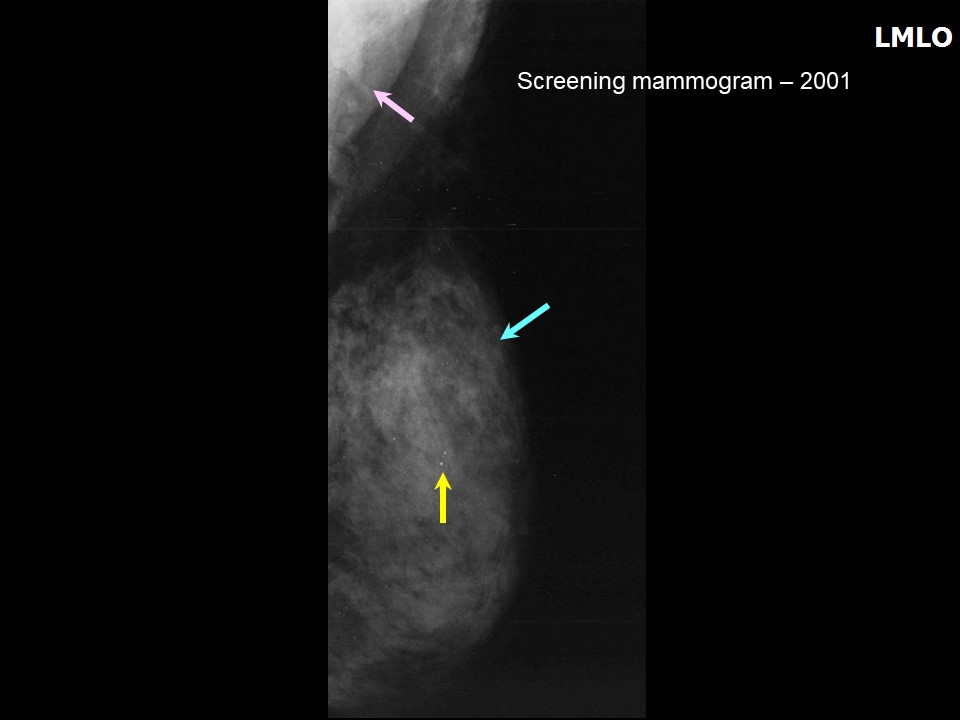 |
| Breast composition: | ACR category c (the breasts are heterogeneously dense, which may obscure small masses) | Mammography features: |
| ‣ Location of the lesion: | June 2001: Left breast, upper outer quadrant at 12 oclock, middle third |
| ‣ Mass: | |
| • Number: | 0 |
| • Size: | None |
| • Shape: | None |
| • Margins: | None |
| • Density: | None |
| ‣ Calcifications: | |
| • Typically benign: | Typically benign |
| • Suspicious: | None |
| • Distribution: | None |
| ‣ Architectural distortion: | None |
| ‣ Asymmetry: | None |
| ‣ Intramammary node: | None |
| ‣ Skin lesion: | None |
| ‣ Solitary dilated duct: | None |
| ‣ Associated features: | None |
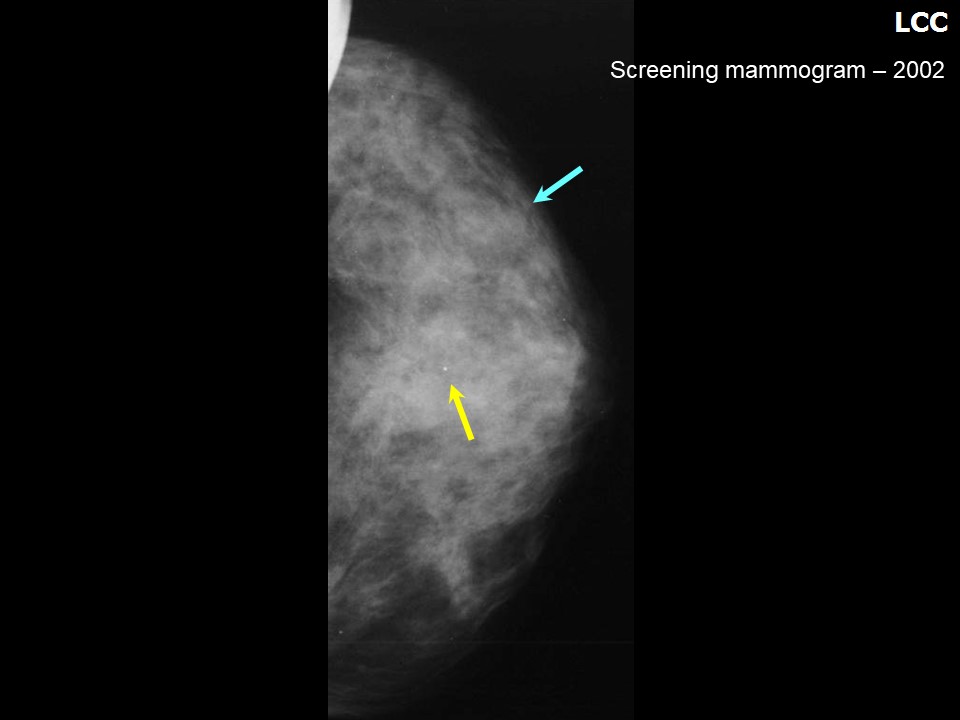 | 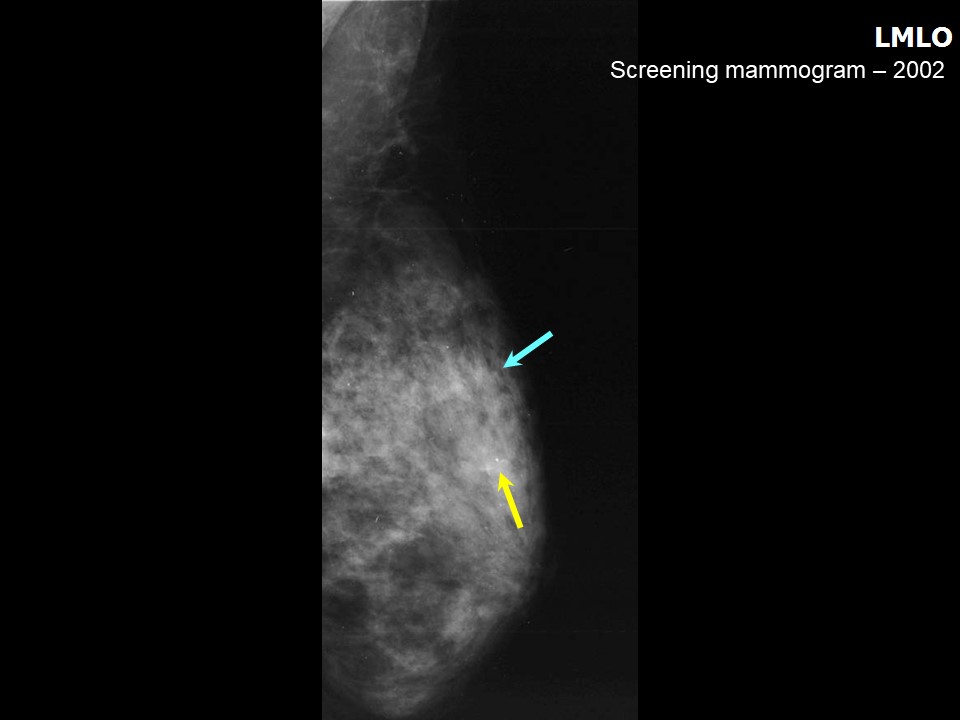 |
| Breast composition: | ACR category c (the breasts are heterogeneously dense, which may obscure small masses) | Mammography features: |
| ‣ Location of the lesion: | 2002: Left breast, upper outer quadrant at 12 oclock, middle third |
| ‣ Mass: | |
| • Number: | 0 |
| • Size: | None |
| • Shape: | None |
| • Margins: | None |
| • Density: | None |
| ‣ Calcifications: | |
| • Typically benign: | Stable benign calcifications on mammography dated 2002 |
| • Suspicious: | None |
| • Distribution: | None |
| ‣ Architectural distortion: | None |
| ‣ Asymmetry: | None |
| ‣ Intramammary node: | None |
| ‣ Skin lesion: | None |
| ‣ Solitary dilated duct: | None |
| ‣ Associated features: | None |
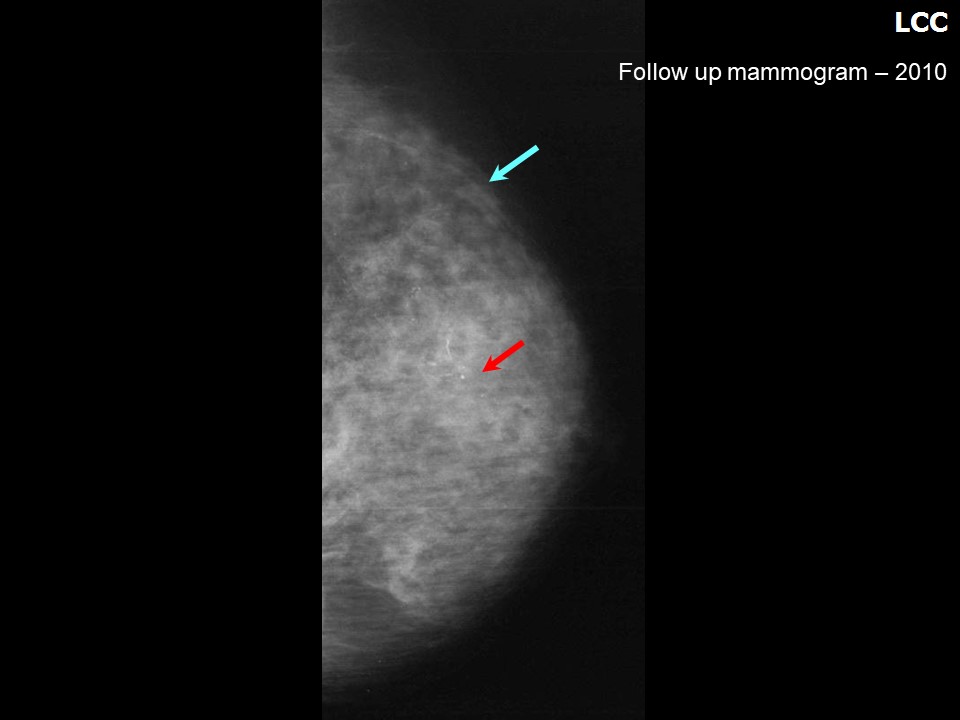 | 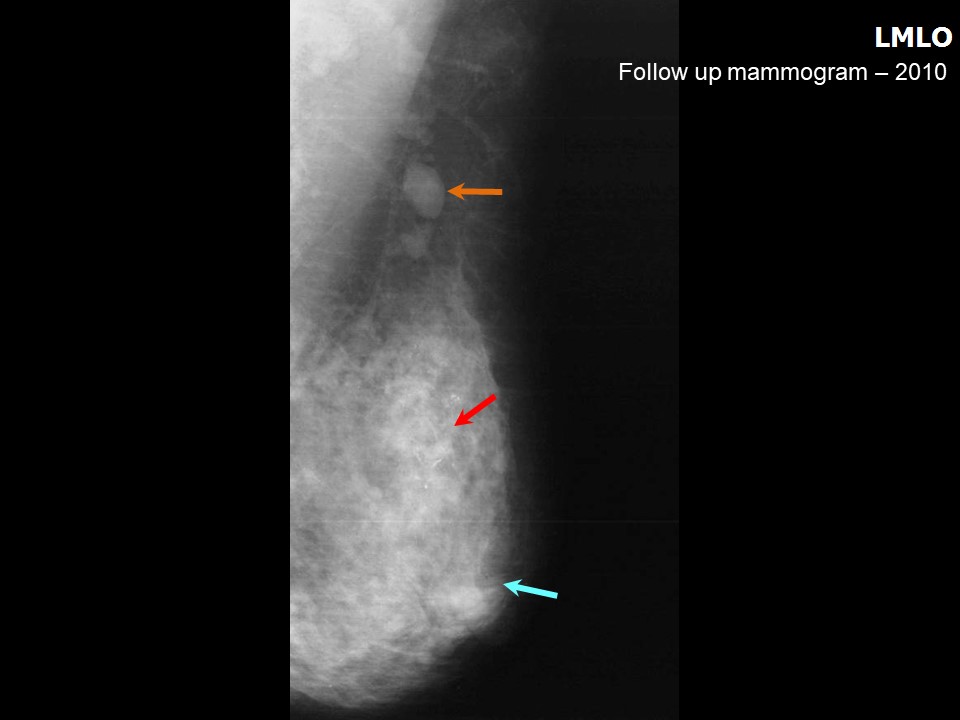 |
| Breast composition: | ACR category c (the breasts are heterogeneously dense, which may obscure small masses) | Mammography features: |
| ‣ Location of the lesion: | 2010: Left breast, upper outer quadrant at 12 oclock, middle third |
| ‣ Mass: | |
| • Number: | 1 |
| • Size: | Not measurable in the dense parenchyma |
| • Shape: | Irregular |
| • Margins: | Indistinct |
| • Density: | High |
| ‣ Calcifications: | |
| • Typically benign: | None |
| • Suspicious: | Fine-linear branching (new finding: interval change noted) |
| • Distribution: | Regional |
| ‣ Architectural distortion: | Present |
| ‣ Asymmetry: | Present |
| ‣ Intramammary node: | Present |
| ‣ Skin lesion: | None |
| ‣ Solitary dilated duct: | None |
| ‣ Associated features: | Axillary lymphadenopathy |
Ultrasound:
 |  |
 |
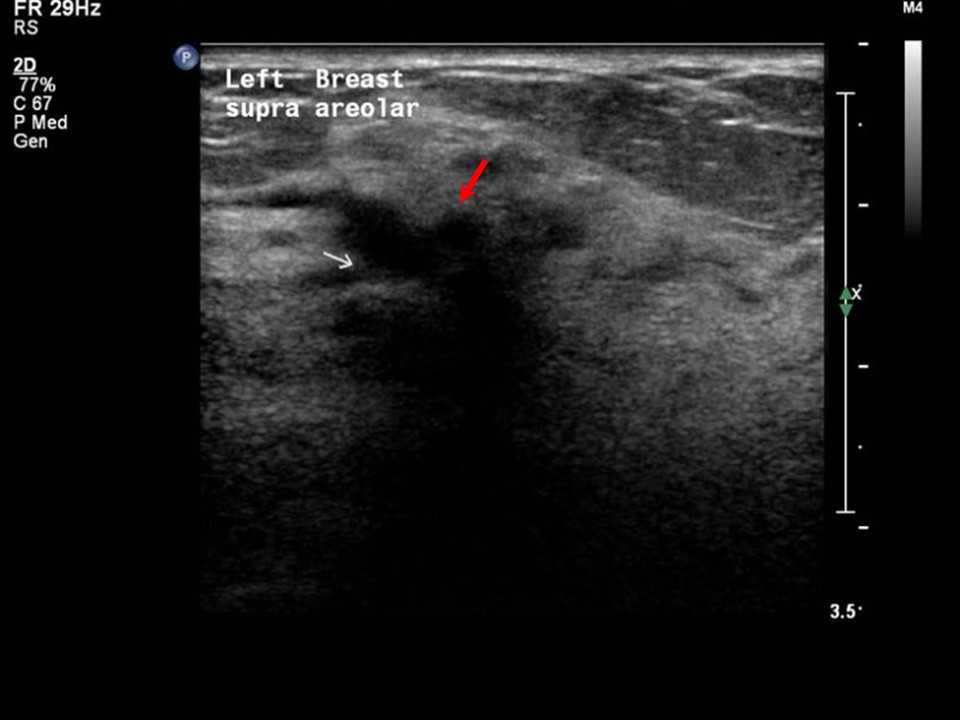
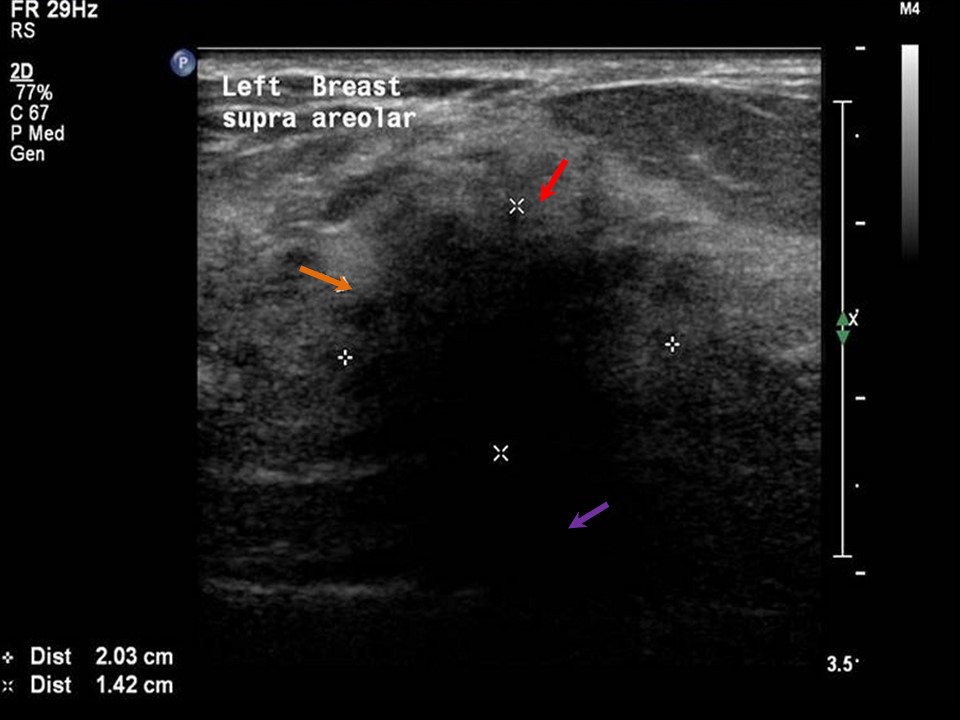
| Ultrasound features: Left breast, central portion of the breast at 2 oclock position along superior areolar margin | |
| ‣ Mass | |
| • Location: | Left breast, central portion of the breast at 2 oclock position along superior areolar margin |
| • Number: | 1 |
| • Size: | 2.03 × 1.42 cm |
| • Shape: | Irregular |
| • Orientation: | Not parallel |
| • Margins: | Spiculated |
| • Echo pattern: | Hypoechoic |
| • Posterior features: | Posterior shadowing |
| ‣ Calcifications: | None |
| ‣ Associated features: | Lymphadenopathy axillary, architectural distortion, and internal vascularity |
| ‣ Special cases: | None |
BI-RADS:
BI-RADS Category (2001): 2 (benign)BI-RADS Category (2002): 2 (benign)
BI-RADS Category (2010): 5 (highly suggestive of malignancy)
Further assessment:
Further assessment advised: Referral for cytologyCytology:
 |
| Cytology features: | |
| ‣ Type of sample: | Nipple discharge |
| ‣ Site of biopsy: | |
| • Laterality: | Left |
| • Quadrant: | |
| • Localization technique: | Nipple discharge |
| • Nature of aspirate: | Clear sticky fluid |
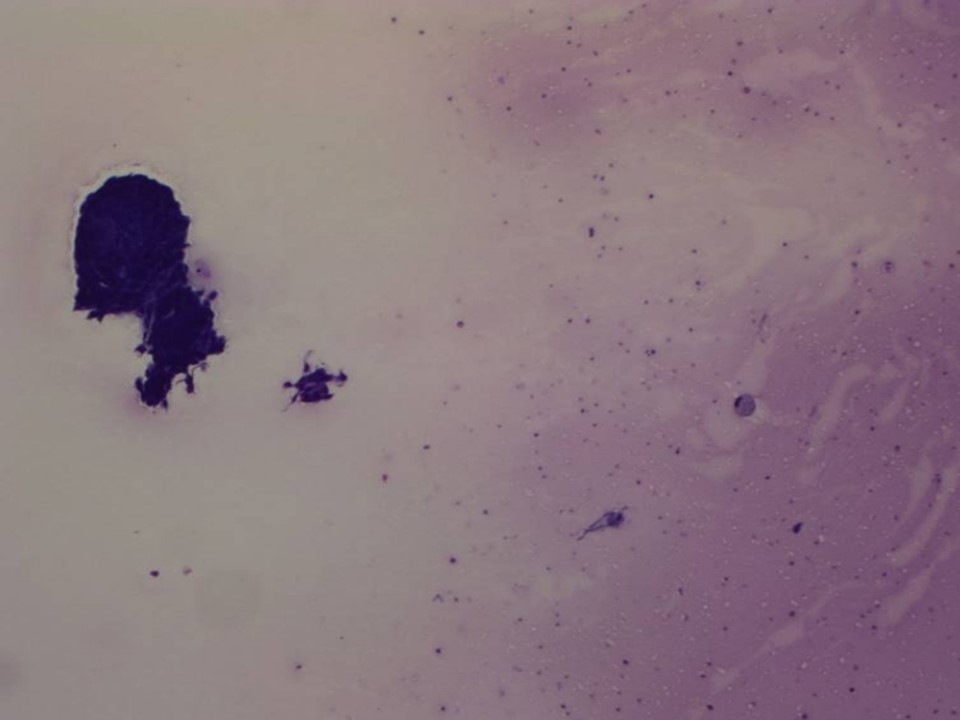
| ‣ Cytological description: | Malignant ductal cells with foamy macrophages on a thick proteinaceous fluid background |
| ‣ Reporting category: | Malignant |
| ‣ Diagnosis: | Carcinoma |
| ‣ Comments: | None |
 |
| Cytology features: | |
| ‣ Type of sample: | Ultrasound-guided FNAC breast lump |
| ‣ Site of biopsy: | |
| • Laterality: | Left |
| • Quadrant: | Upper outer |
| • Localization technique: | Ultrasound-guided |
| • Nature of aspirate: | Whitish |
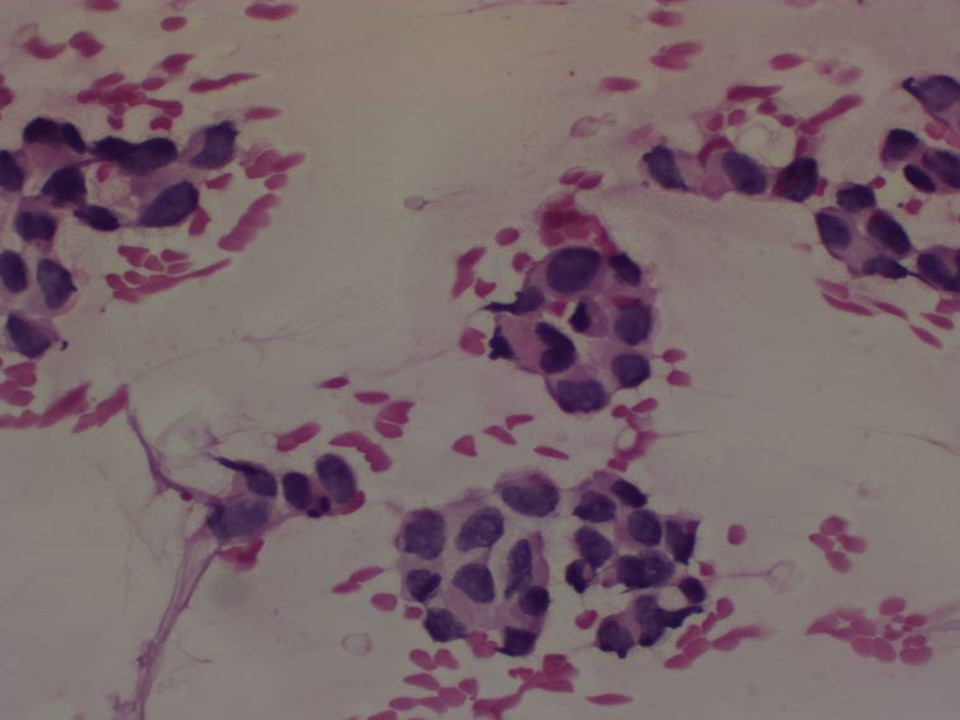
| ‣ Cytological description: | Pleomorphic malignant cells present. Background shows foamy macrophages and proteinaceous fluid |
| ‣ Reporting category: | Malignant |
| ‣ Diagnosis: | Carcinoma |
| ‣ Comments: | None |
 |
| Cytology features: | |
| ‣ Type of sample: | Ultrasound-guided FNAC left axillary lymph node |
| ‣ Site of biopsy: | |
| • Laterality: | Left |
| • Quadrant: | Left axilla |
| • Localization technique: | Ultrasound-guided |
| • Nature of aspirate: | Whitish |
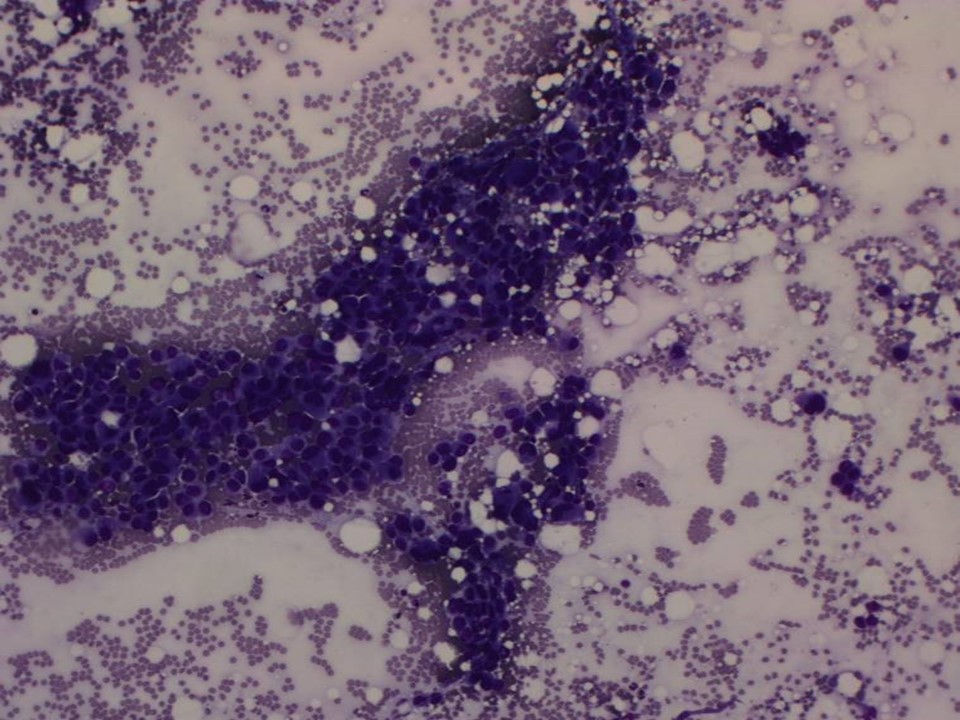
| ‣ Cytological description: | Malignant ductal cells with lymphocytes in the background |
| ‣ Reporting category: | Malignant |
| ‣ Diagnosis: | Metastases in node |
| ‣ Comments: | None |
Histopathology:
MRM
 | 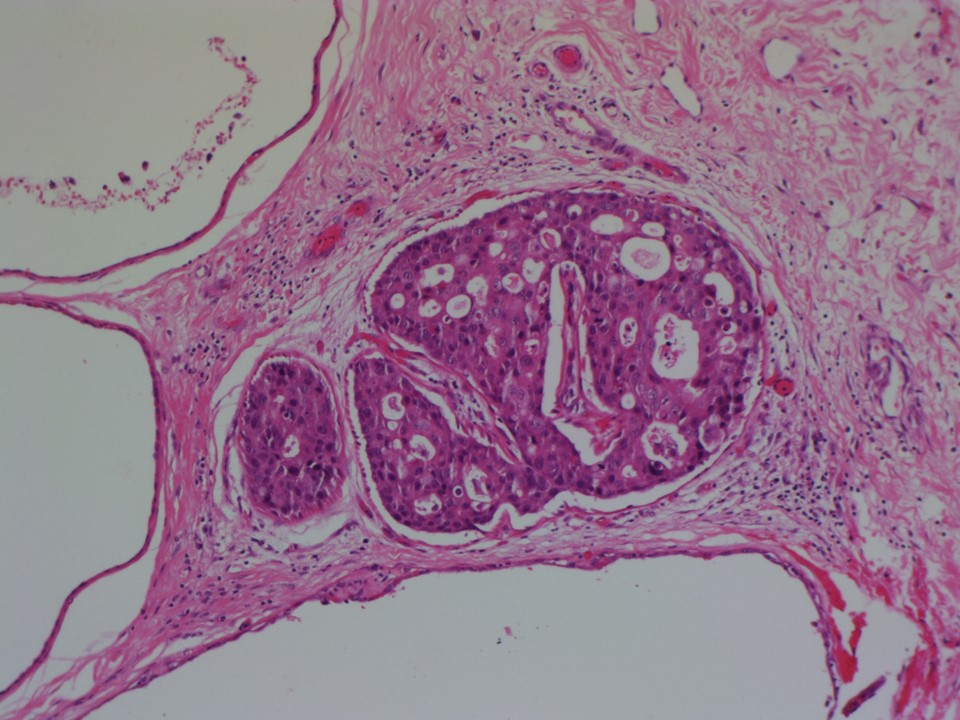 |
| Histopathology features: | |
| ‣ Specimen type: | MRM |
| ‣ Laterality: | Left |
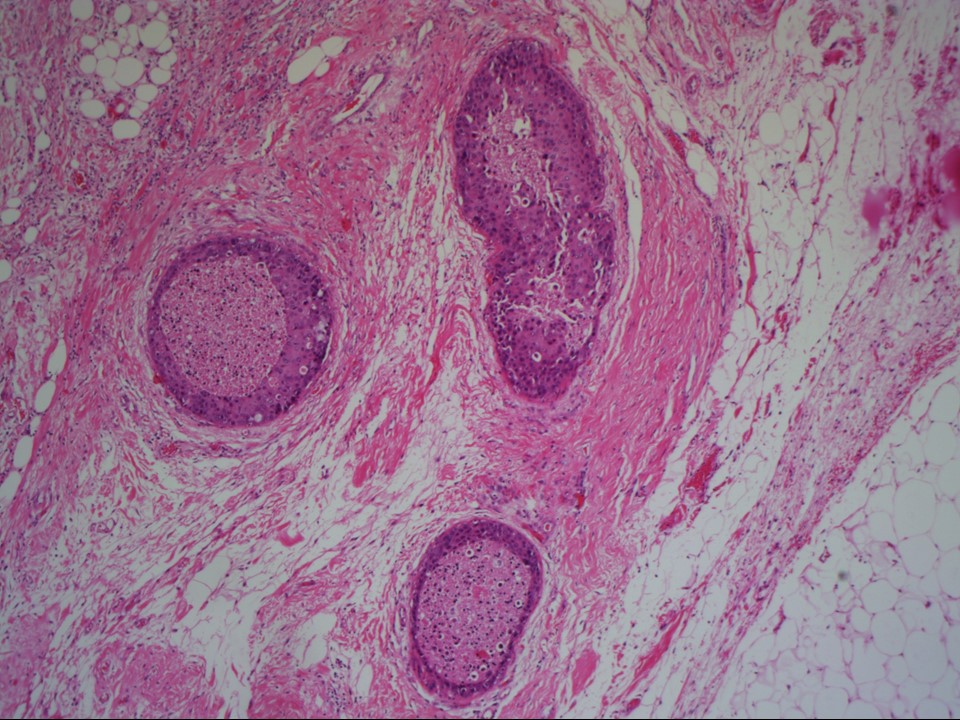
| ‣ Macroscopy: | Specimen (16.0 × 15.0 × 5.0 cm) with overlying skin flap (12.5 × 9.5 cm). The nipple and areola are unremarkable. A linear scar (0.6 × 0.2 cm) is located in the upper outer quadrant. Cut surface shows extensive greyish white areas with two firm to hard nodules (2.5 × 2.0 × 1.5 cm and 2.0 × 1.5 × 1.2 cm) in the central and upper quadrants. They are located 2.5 cm from the skin and 0.4 cm from the base |
| ‣ Histological type: | No invasive carcinoma is identified in the extensively sampled specimen |
| ‣ Histological grade: | |
| ‣ Mitosis: | |
| ‣ Maximum invasive tumour size: | |
| ‣ Lymph node status: | 0/21 |
| ‣ Peritumoural lymphovascular invasion: | Absent |
| ‣ DCIS/EIC: | EIC is identified of solid, cribriform, and comedo type DCIS, with high nuclear grade and central necrosis. The DCIS is located in the upper quadrant, central region as well as in the axillary tail |
| ‣ Margins: | Free of tumour |
| ‣ Pathological stage: | pTisN0 |
| ‣ Biomarkers: | ER positive and PR positive in DCIS |
| ‣ Comments: | Adjacent breast shows multiple intraductal papillomas, stromal fibrosis, and ectatic ducts. In view of findings of only EIC and no invasive carcinoma in the MRM specimen, the FNAC from the axillary node should be interpreted as ductal carcinoma cells arising from DCIS involving the axillary tail because all the axillary nodes on histopathology are free of tumour |
Case summary:
| Postmenopausal woman with increased risk of developing breast cancer presented with left nipple discharge. Examination revealed a small area of irregular thickening on the left breast. Mammography and breast ultrasound dated 2010 reveal a new spiculated mass lesion and pleomorphic microcalcifications in the left breast. Compared with previous mammograms dated 2001 and 2002, follow-up reveals developing asymmetry in the left breast. Interval change is seen. Diagnosed as highly suggestive of malignancy, BI-RADS 5 on imaging, cytology of nipple discharge, breast lump, and the axillary lump suggestive of carcinoma and EIC in the left breast and axillary tail, with no invasive carcinoma, pTisN0 on histopathology. |
Learning points:
|