



Home / Training / Manuals / Atlas of breast cancer early detection / Cases
Atlas of breast cancer early detection
Filter by language: English / Русский
Go back to the list of case studies
.png) Click on the pictures to magnify and display the legends
Click on the pictures to magnify and display the legends
BI-RADS Category (2013): 5 (highly suggestive of malignancy)
| Case number: | 098 |
| Age: | 62 |
| Clinical presentation: | Postmenopausal woman, presented with a painful left breast lump of duration 1 month. She had increased risk of developing breast cancer because of family history. Examination revealed small lumps in the upper outer quadrant of the left breast. |
Mammography:
 |  |
| Breast composition: | ACR category c (the breasts are heterogeneously dense, which may obscure small masses) | Mammography features: |
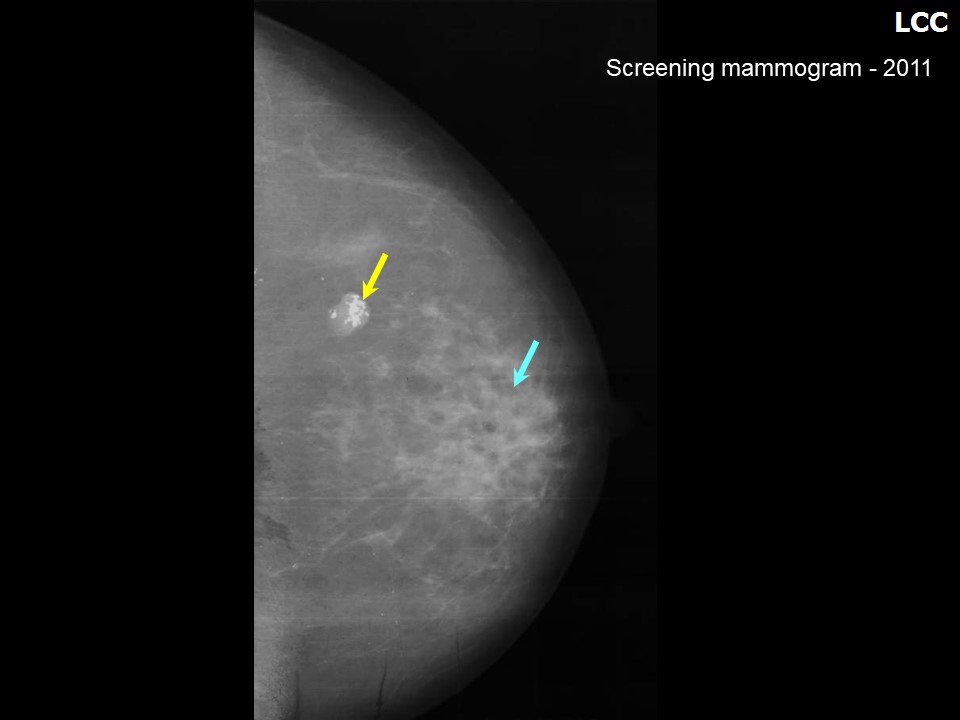
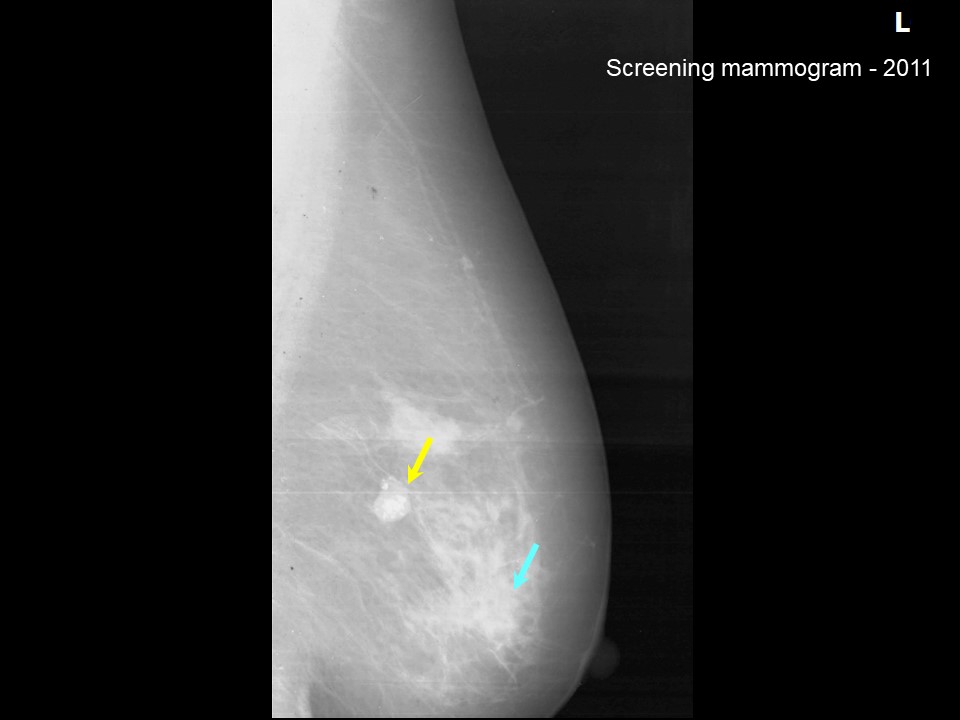
| ‣ Location of the lesion: | Screening mammogram dated 2011: Left breast, upper outer quadrant at 1 oclock, posterior third |
| ‣ Mass: | |
| • Number: | 1 |
| • Size: | 1.5 cm in greatest dimension |
| • Shape: | Oval |
| • Margins: | Circumscribed |
| • Density: | Equal |
| ‣ Calcifications: | |
| • Typically benign: | Popcorn-like |
| • Suspicious: | None |
| • Distribution: | None |
| ‣ Architectural distortion: | None |
| ‣ Asymmetry: | None |
| ‣ Intramammary node: | None |
| ‣ Skin lesion: | None |
| ‣ Solitary dilated duct: | None |
| ‣ Associated features: | Typically benign, coarse, popcorn-like calcifications |
 |  |
 |
| Breast composition: | ACR category b (there are scattered areas of fibroglandular density) | Mammography features: |
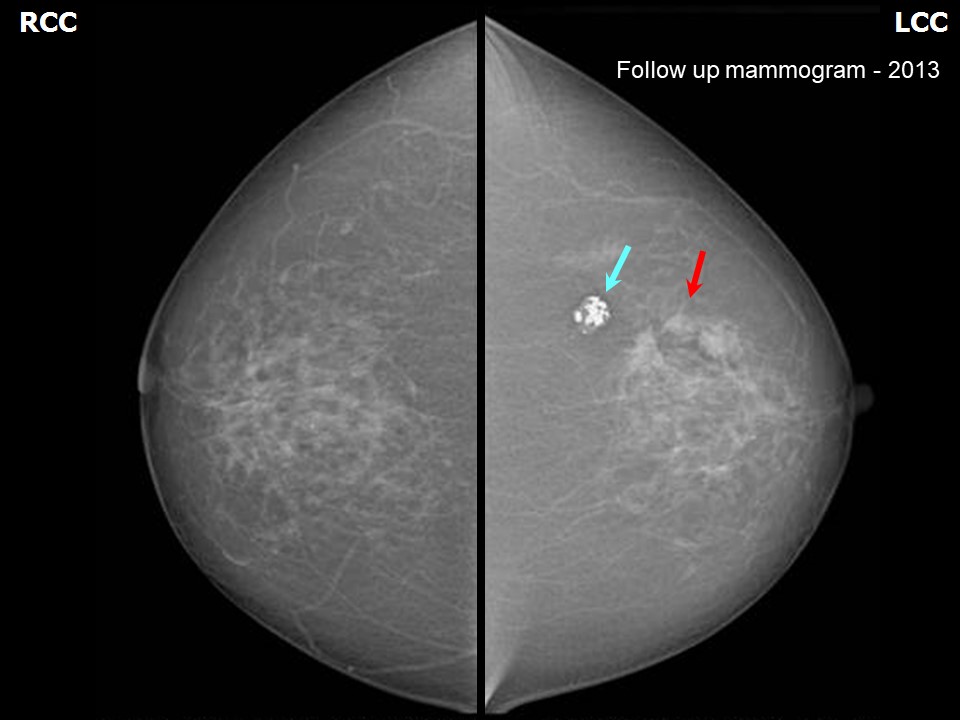
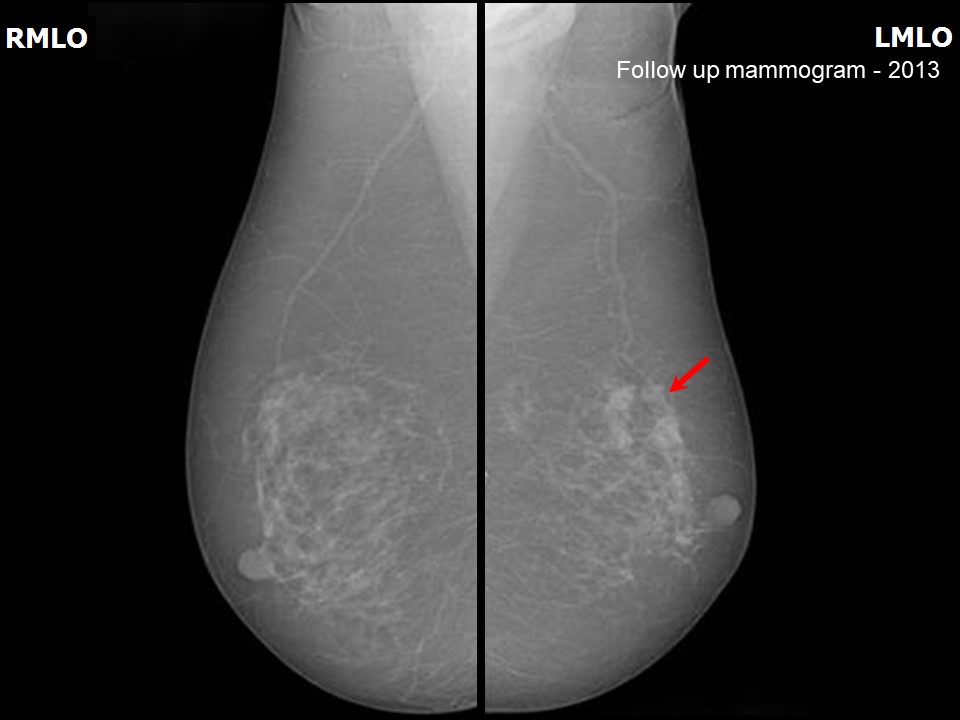
| ‣ Location of the lesion: | Follow-up mammogram dated 2013: Left breast, upper outer quadrant at 1 oclock, middle third |
| ‣ Mass: | |
| • Number: | 3 (this is a new finding, developing asymmetry). Stable lesion of 2011, 1.2 cm size with popcorn calcification also seen at 1oclock position |
| • Size: | 3 masses: 1.6 cm, 1.0 cm, and 0.77 cm in greatest dimension |
| • Shape: | Irregular |
| • Margins: | Spiculated |
| • Density: | High |
| ‣ Calcifications: | |
| • Typically benign: | None |
| • Suspicious: | Fine pleomorphic |
| • Distribution: | None |
| ‣ Architectural distortion: | Present |
| ‣ Asymmetry: | Focal |
| ‣ Intramammary node: | None |
| ‣ Skin lesion: | None |
| ‣ Solitary dilated duct: | None |
| ‣ Associated features: | Trabecular thickening, architectural distortion, and fine pleomorphic microcalcifications |
Ultrasound:
 |
| Ultrasound features: 2011: Left breast, upper outer quadrant at 1 oclock | |
| ‣ Mass | |
| • Location: | 2011: Left breast, upper outer quadrant at 1 oclock |
| • Number: | 1 |
| • Size: | 1.5 cm |
| • Shape: | Oval |
| • Orientation: | Parallel |
| • Margins: | Circumscribed |
| • Echo pattern: | Dense macrocalcifications |
| • Posterior features: | Posterior shadowing |
| ‣ Calcifications: | Typically benign in mass |
| ‣ Associated features: | Calcifications in mass |
| ‣ Special cases: | None |
 |  |
 |
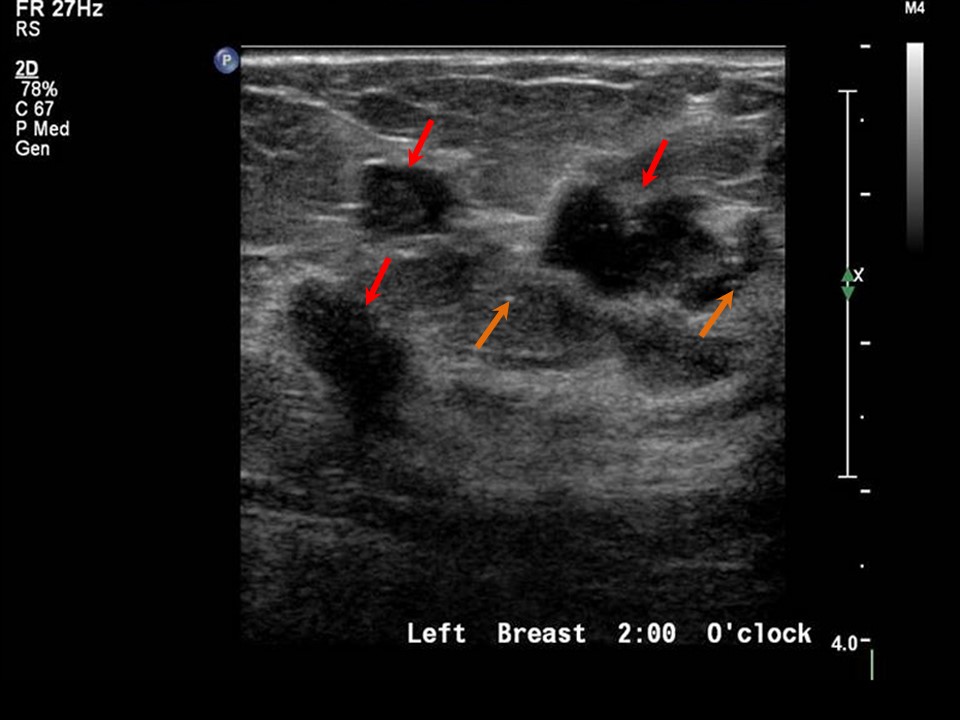
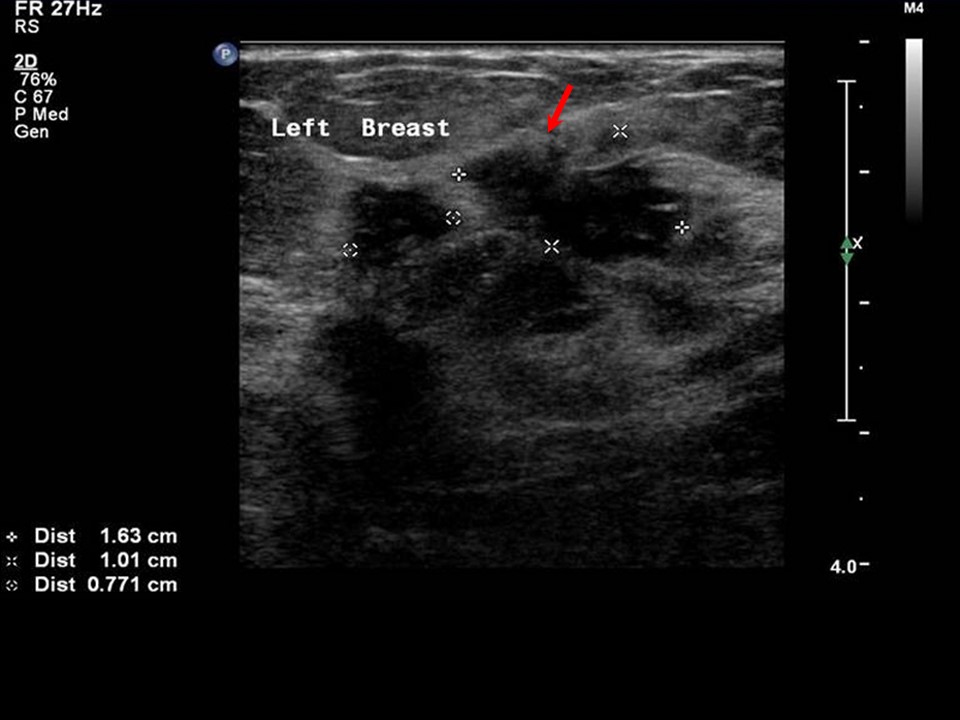
| Ultrasound features: Follow-up 2013: Left breast, upper outer quadrant at 1 oclock | |
| ‣ Mass | |
| • Location: | Follow-up 2013: Left breast, upper outer quadrant at 1 oclock |
| • Number: | 3 (this is new finding, developing asymmetry). Stable lesion of 2011 with popcorn-like calcification also seen at 1 oclock |
| • Size: | 1.6 x 1.0 x 0.7 cm in greatest dimension |
| • Shape: | Irregular |
| • Orientation: | Not parallel |
| • Margins: | Spiculated |
| • Echo pattern: | Hypoechoic |
| • Posterior features: | No posterior features |
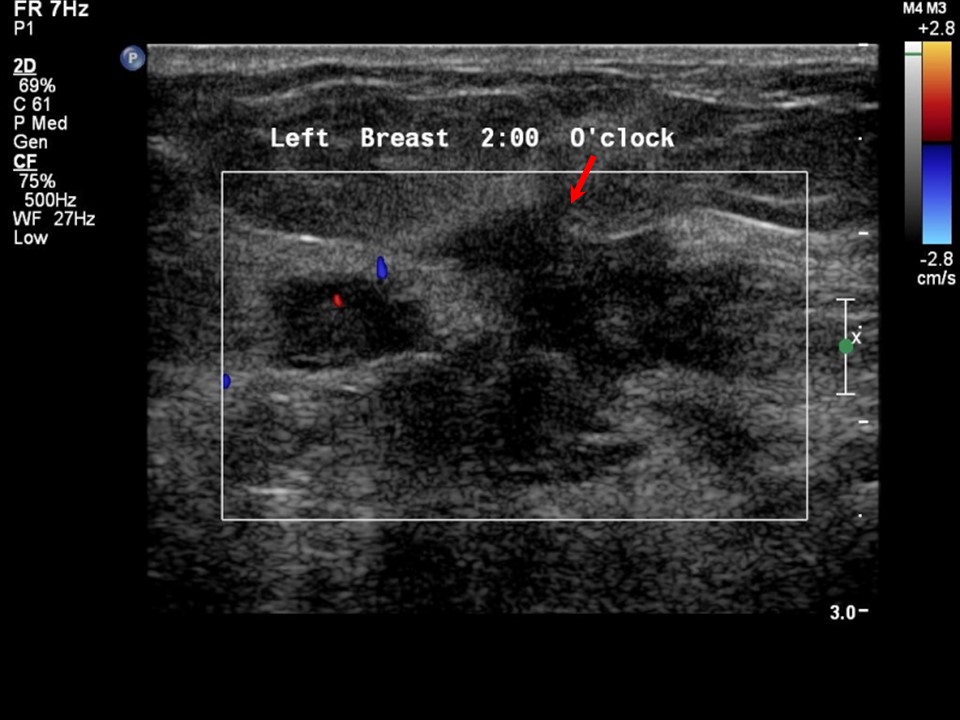
| ‣ Calcifications: | Microcalcifications in mass and adjacent parenchyma |
| ‣ Associated features: | Architectural distortion and internal vascularity |
| ‣ Special cases: | None |
BI-RADS:
BI-RADS Category (2011): 2 (benign)BI-RADS Category (2013): 5 (highly suggestive of malignancy)
Further assessment:
Further assessment advised: Referral for cytologyCytology:
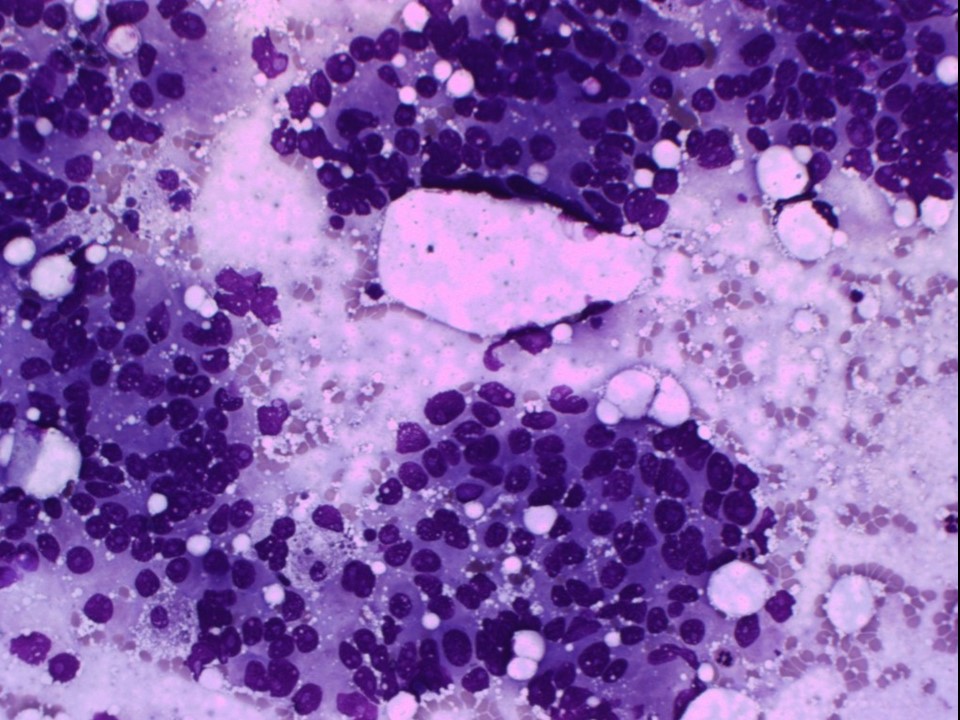 |
| Cytology features: | |
| ‣ Type of sample: | FNAC (solid lesion) |
| ‣ Site of biopsy: | |
| • Laterality: | Left |
| • Quadrant: | Upper outer |
| • Localization technique: | Palpation |
| • Nature of aspirate: | Whitish |
| ‣ Cytological description: | Smear shows many loosely cohesive clusters and many dissociated cells. Individuals cells are large and have a high N:C ratio. Nucleus is hyperchromatic and shows coarsely granular to clumped chromatin and prominent nucleoli. Foam cells are seen in background |
| ‣ Reporting category: | Malignant |
| ‣ Diagnosis: | Carcinoma |
| ‣ Comments: | None |
Histopathology:
MRM
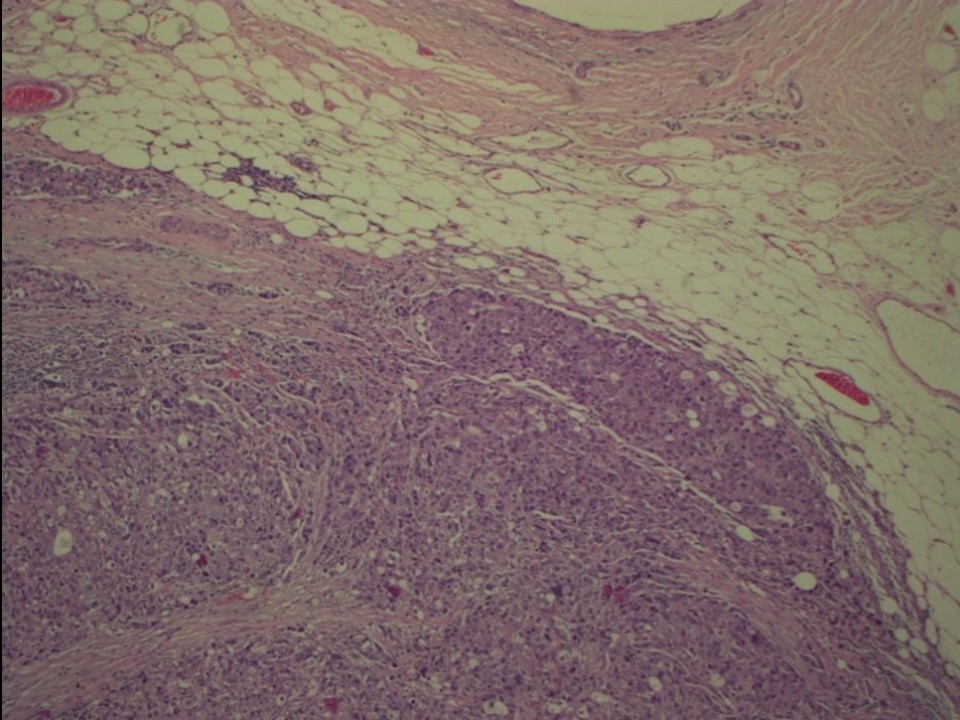 | 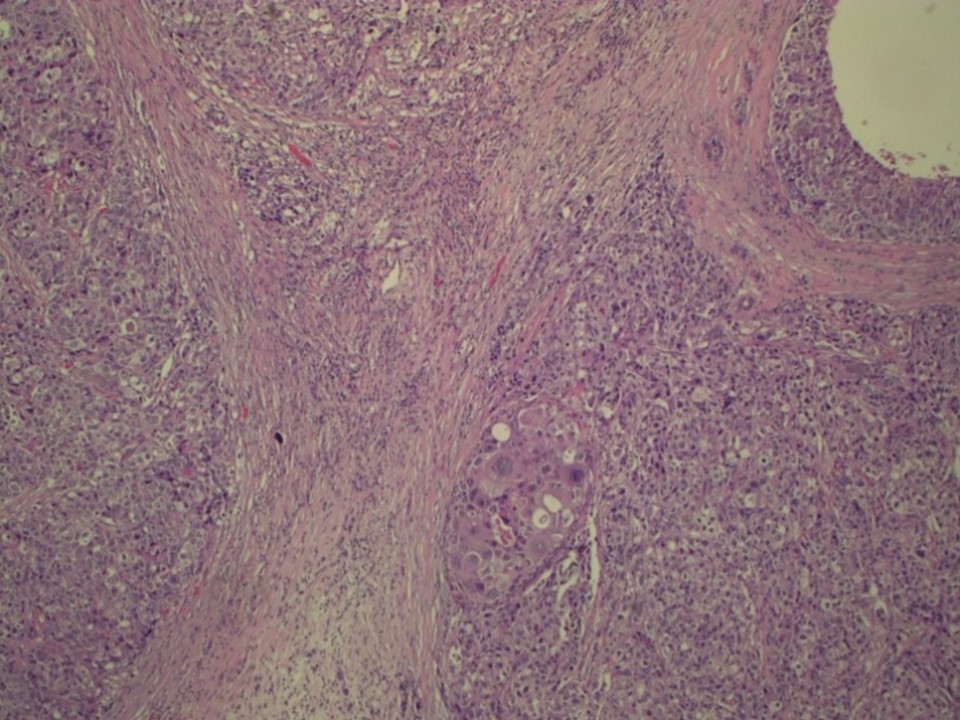 |
| Histopathology features: | |
| ‣ Specimen type: | MRM |
| ‣ Laterality: | Left |
| ‣ Macroscopy: | On serial sectioning, two firm greyish white areas are identified, 1.7 × 1.6 × 2.0 cm and 2.0 × 1.8 × 1.5 cm, located in the upper outer quadrant and 1.5 cm from each other. The lesion is located > 3.0 cm from the skin and 1.8 cm from the base. Whitish fibrotic areas are seen in the remaining breast tissue |
| ‣ Histological type: | Invasive carcinoma of no special type |
| ‣ Histological grade: | Grade 3 (3 + 3 + 2 = 8) |
| ‣ Mitosis: | 16 |
| ‣ Maximum invasive tumour size: | Largest 2.0 cm; the second nodule was 1.7 cm |
| ‣ Lymph node status: | 0/24 |
| ‣ Peritumoural lymphovascular invasion: | Not identified |
| ‣ DCIS/EIC: | Not identified |
| ‣ Margins: | Free of tumour |
| ‣ Pathological stage: | pT1c(2)N0 |
| ‣ Biomarkers: | |
| ‣ Comments: |
Case summary:
| Postmenopausal woman with increased risk of developing breast cancer presented with a painful left breast lump of duration 1 month. Mammograms and breast ultrasound results from 2013 showed new suspicious irregular lesions in the left breast with pleomorphic microcalcifications and fine linear calcifications in segmental distribution, along with the masses. Compared with previous mammograms from 2011, follow-up reveals developing asymmetries in the left breast. The previously seen partially calcified fibroadenoma in the upper outer quadrant of the left breast is stable. Interval change is seen. Diagnosed as highly suggestive of malignancy, BI-RADS 5 on imaging, as carcinoma on cytology, and as invasive breast carcinoma of no special type, pT1c(2)N0 on histopathology. |
Learning points:
|