



Home / Training / Manuals / Atlas of breast cancer early detection / Cases
Atlas of breast cancer early detection
Go back to the list of case studies
.png) Click on the pictures to magnify and display the legends
Click on the pictures to magnify and display the legends
BI-RADS Category (MRI Bi-RADS): 5 (highly suggestive of malignancy)
| Case number: | 093 |
| Age: | 66 |
| Clinical presentation: | Postmenopausal woman with average risk of developing breast cancer presented with a right breast lump. She says she has had the right breast lump for 20 years and that it has increased in size over the last 3 months. There is no nipple discharge or overlying skin changes. |
 |
Mammography:
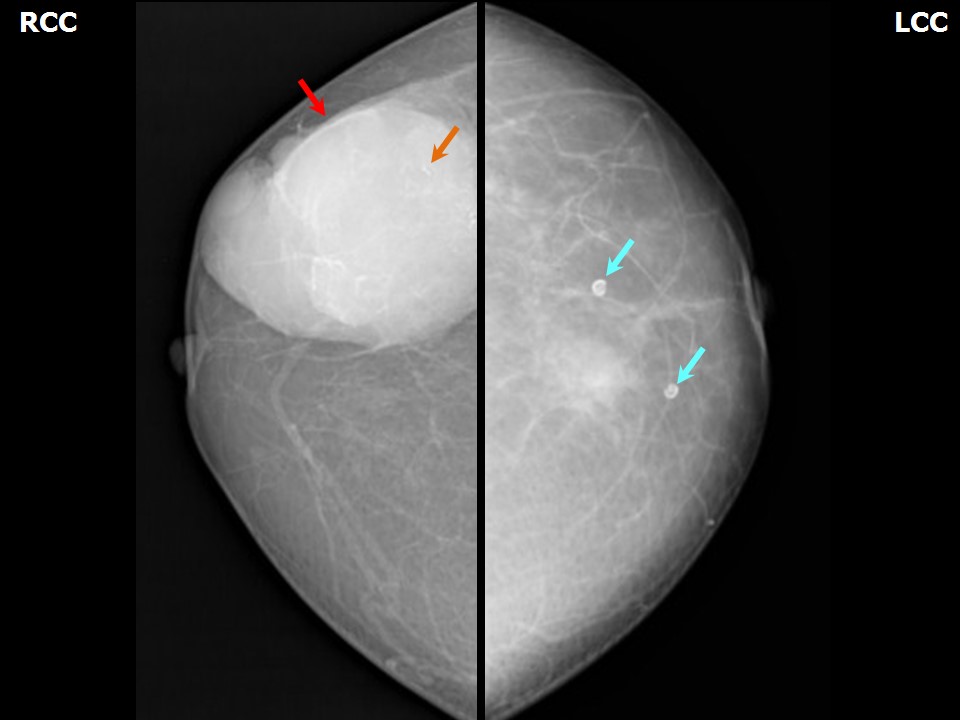 | 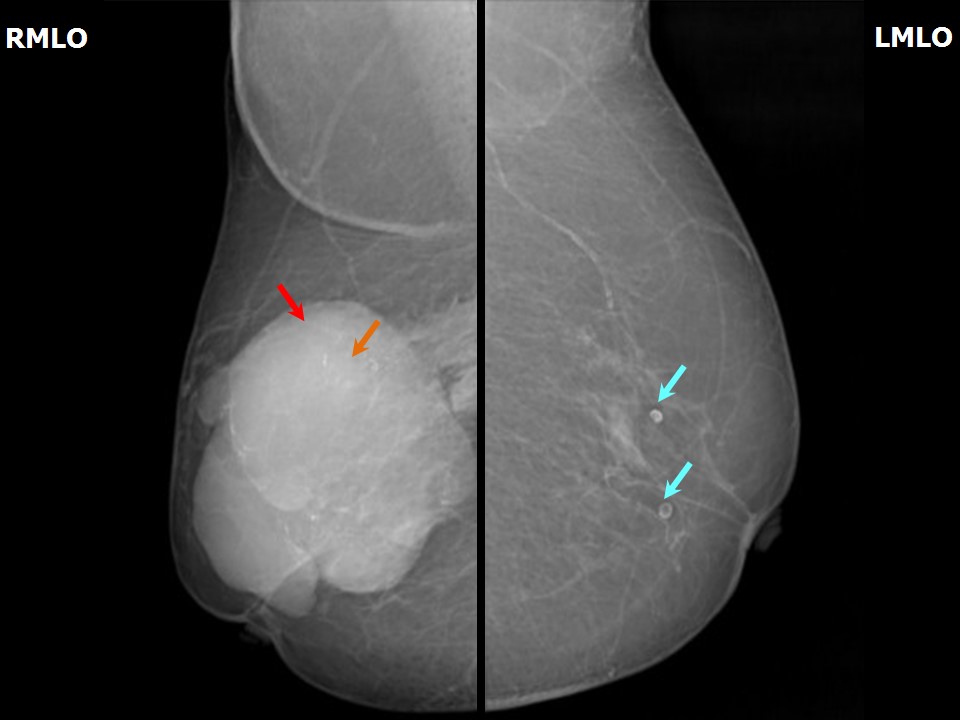 |
| Breast composition: | ACR category a (the breasts are almost entirely fatty) | Mammography features: |
| ‣ Location of the lesion: | Right breast, upper outer quadrant at 911 oclock, anterior, middle, and posterior thirds |
| ‣ Mass: | |
| • Number: | 1 |
| • Size: | 8.2 × 7.7 × 6.7 cm |
| • Shape: | Irregular |
| • Margins: | circumscribed |
| • Density: | High |
| ‣ Calcifications: | |
| • Typically benign: | None |
| • Suspicious: | Fine linear or fine linear branching |
| • Distribution: | Linear |
| ‣ Architectural distortion: | None |
| ‣ Asymmetry: | None |
| ‣ Intramammary node: | None |
| ‣ Skin lesion: | None |
| ‣ Solitary dilated duct: | None |
| ‣ Associated features: | Calcifications |
| Breast composition: | ACR category a (the breasts are almost entirely fatty) | Mammography features: |
| ‣ Location of the lesion: | Left breast, central quadrant, anterior and middle thirds |
| ‣ Mass: | |
| • Number: | 0 |
| • Size: | None |
| • Shape: | None |
| • Margins: | None |
| • Density: | None |
| ‣ Calcifications: | |
| • Typically benign: | Round, rim, vascular |
| • Suspicious: | None |
| • Distribution: | Diffuse |
| ‣ Architectural distortion: | None |
| ‣ Asymmetry: | None |
| ‣ Intramammary node: | None |
| ‣ Skin lesion: | None |
| ‣ Solitary dilated duct: | None |
| ‣ Associated features: | None |
Ultrasound:
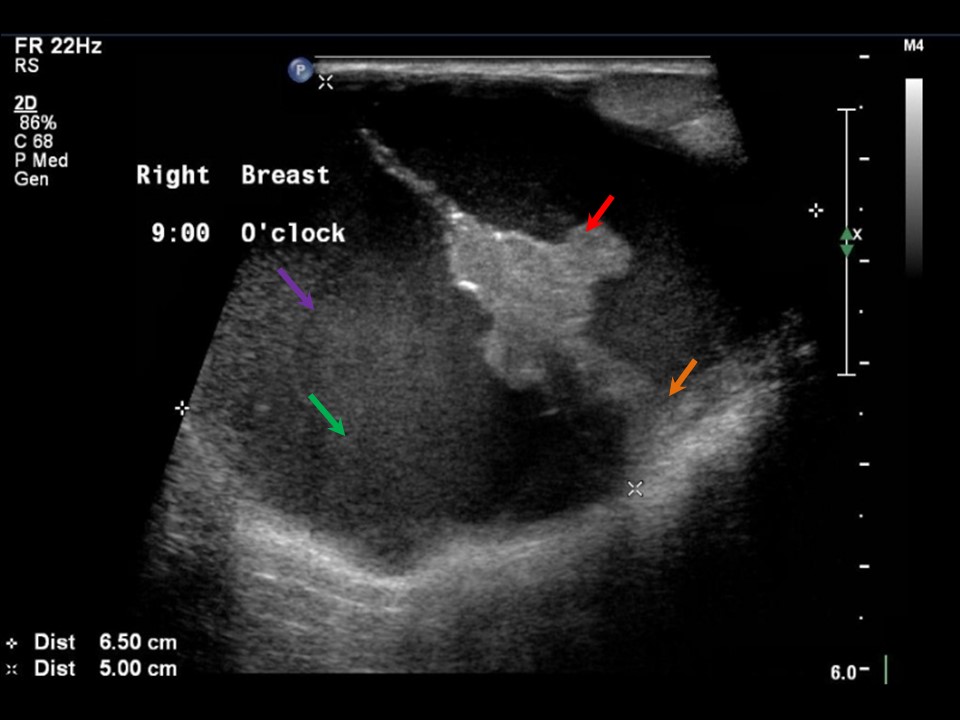 | 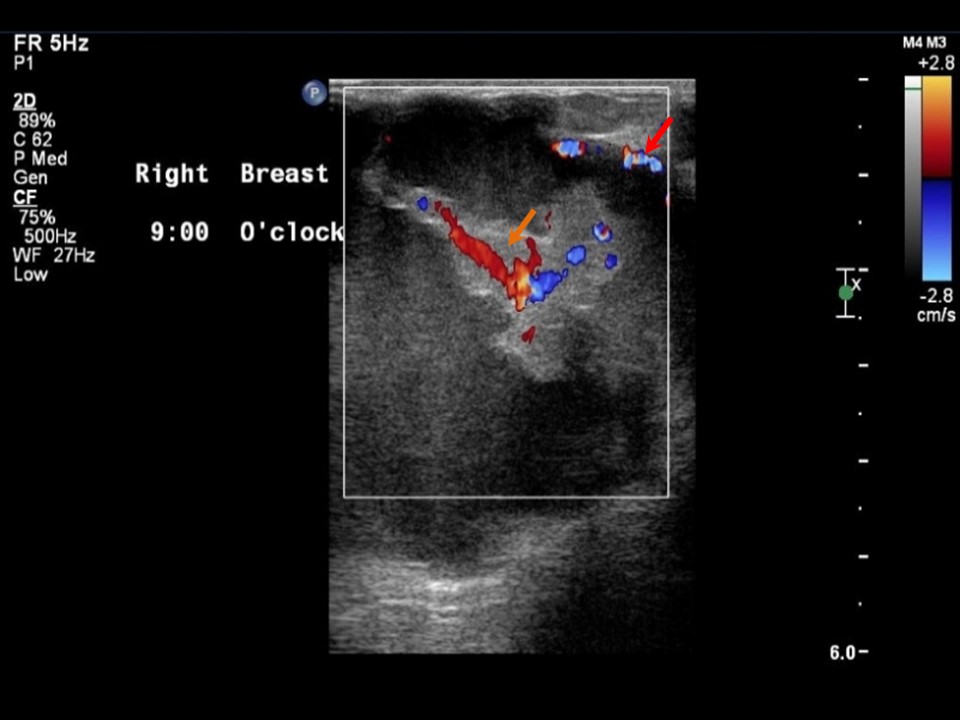 |
| Ultrasound features: Right breast, outer quadrants at 9 oclock | |
| ‣ Mass | |
| • Location: | Right breast, outer quadrants at 9 oclock |
| • Number: | 1 |
| • Size: | 7.0 × 5.0 cm |
| • Shape: | Irregular |
| • Orientation: | Not parallel |
| • Margins: | Circumscribed |
| • Echo pattern: | Complex cystic and solid |
| • Posterior features: | No posterior features |
| ‣ Calcifications: | None |
| ‣ Associated features: | Internal vascularity |
| ‣ Special cases: | None |
BI-RADS:
BI-RADS Category: 5 (highly suggestive of malignancy)BI-RADS Category (MRI Bi-RADS): 5 (highly suggestive of malignancy)
Further assessment:
Further assessment advised: Further imaging with breast MRIMRI:
 | 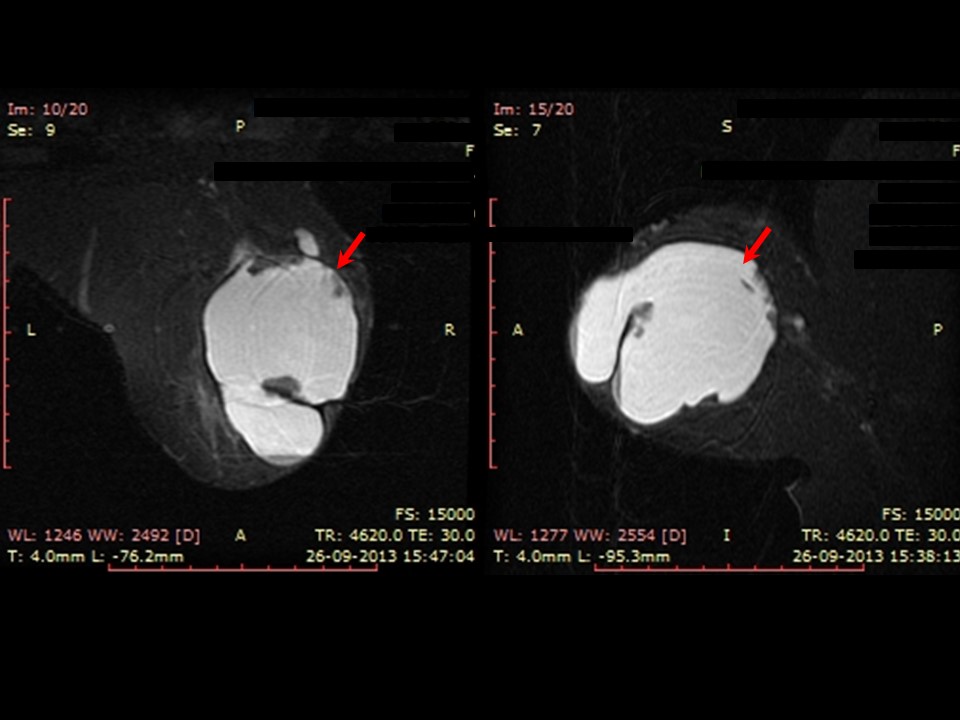 |
| MRI features: | ||
| ‣ MRI features: | Amount of fibroglandular tissue: ACR category b (scattered fibroglandular tissue). Background parenchymal enhancement: Mild (2550%), symmetrical | |
| ‣ Location: | Lateral half of right breast | |
| ‣ Focus: | No | |
| ‣ Mass: | ||
| • Shape: | Oval | |
| • Margin: | Irregular | |
| • Internal enhancement: | Rim enhancement with enhancing septations and enhancing solid components | |
| • Kinetic curve: | Type 3 | |
| ‣ Non-mass enhancement: | ||
| • Distribution: | No | |
| • Internal enhancement: | No | |
| ‣ Non-enhancing findings: | Fluid fluid levels and susceptibility artefacts suggestive of haemorrhage | |
| ‣ Associated features: | Axillary adenopathy | |
| ‣ Axillary nodes: | Enlarged right axillary lymph nodes (largest 1.5 cm) | |
Cytology:
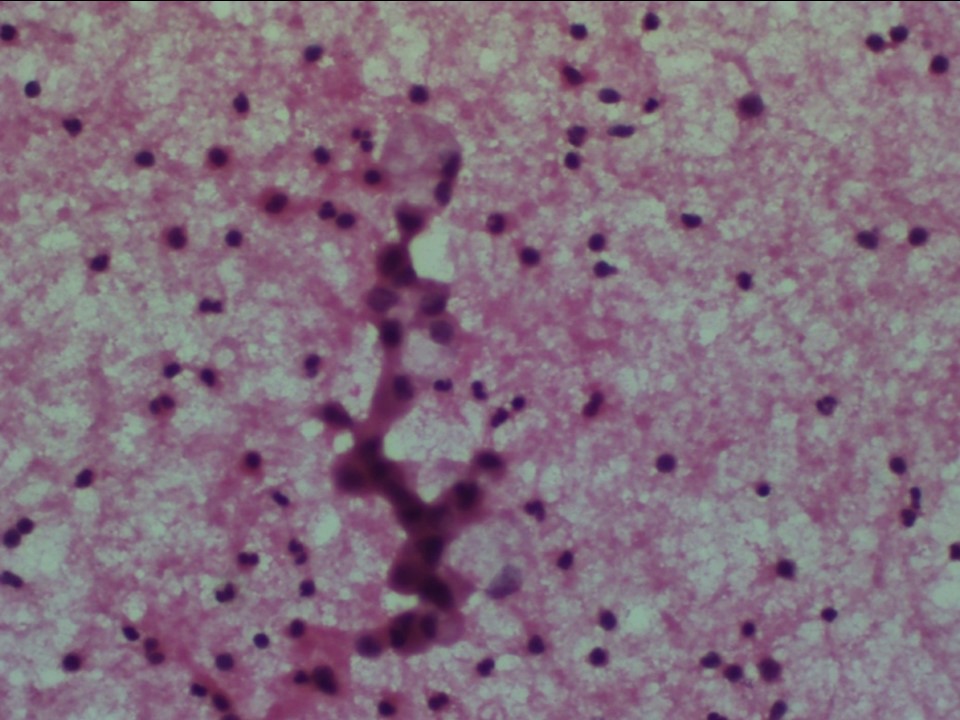 |
| Cytology features: | |
| ‣ Type of sample: | FNAC (cystic lesion) |
| ‣ Site of biopsy: | |
| • Laterality: | Right |
| • Quadrant: | Upper outer |
| • Localization technique: | Palpation |
| • Nature of aspirate: | 12 mL of reddish fluid. Swelling was reduced considerably after, although a small residual nodule was still palpable |
| ‣ Cytological description: | Smears shows mainly RBCs with a few small clusters of benign ductal epithelial cells. A few cells with abundant vacuolated cytoplasm also present |
| ‣ Reporting category: | Benign |
| ‣ Diagnosis: | Consistent with fibrocystic disease |
| ‣ Comments: | Repeat ultrasound-guided FNAC from the solid part advisable |
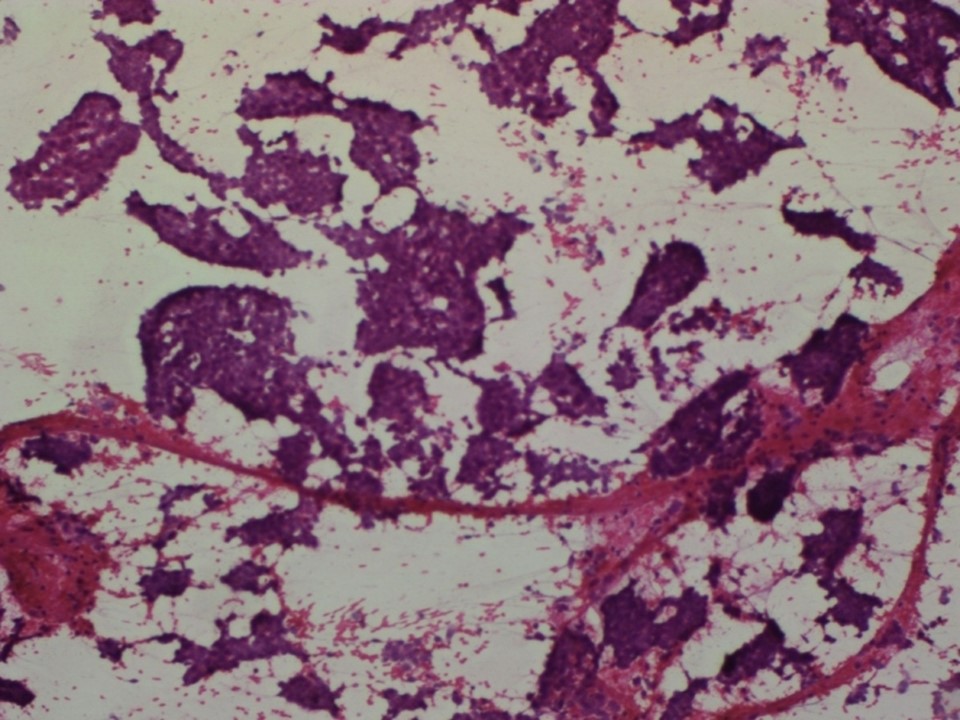 |
| Cytology features: | |
| ‣ Type of sample: | FNAC (solid lesion) |
| ‣ Site of biopsy: | |
| • Laterality: | Right |
| • Quadrant: | Upper outer |
| • Localization technique: | Ultrasound-guided FNAC from right breast lump from solid part of the lesion |
| • Nature of aspirate: | Haemorrhagic |
| ‣ Cytological description: | Smears are cellular and show folded and branching epithelial sheets and finger-like fragments with strands of fibrovascular stroma. These sheets show tightly cohesive benign ductal epithelial cells with dispersed, loosely cohesive epithelial cells seen with mild nuclear atypia |
| ‣ Reporting category: | Atypical, probably benign |
| ‣ Diagnosis: | Papillary lesion of breast with mild nuclear atypia. Tissue diagnosis for further typing advised |
| ‣ Comments: | None |
Histopathology:
Core needle biopsy
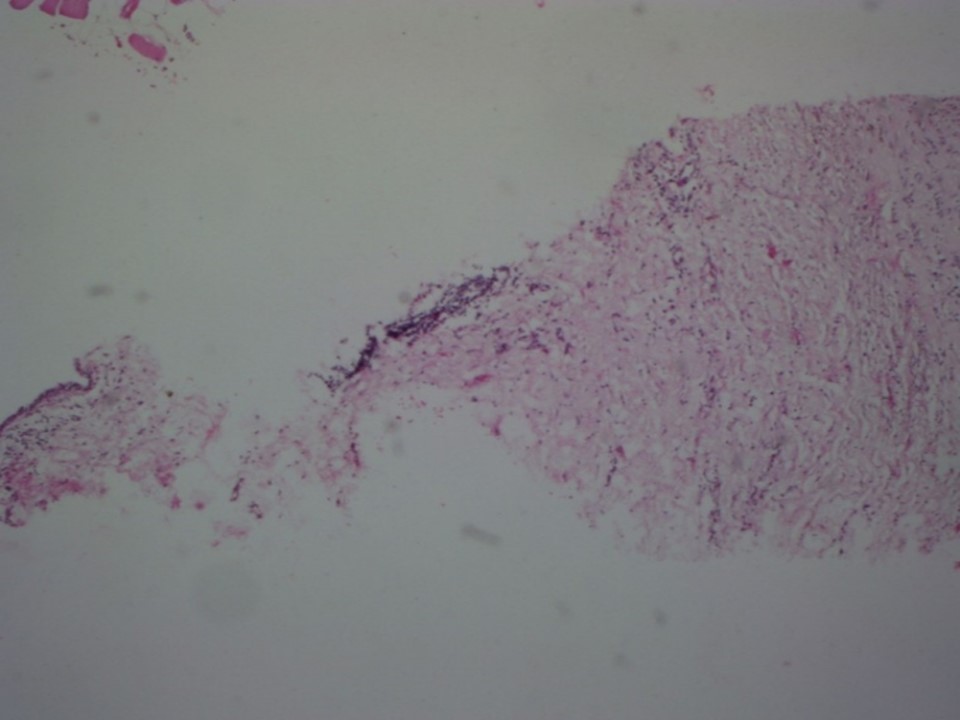 |
| Histopathology features: | |
| ‣ Specimen type: | Core needle biopsy |
| ‣ Laterality: | Right |
| ‣ Macroscopy: | Four small fragmented cores, each < 3 mm in length |
| ‣ Histological type: | Sections through totally submitted tissue reveal fragmented biopsy showing muscle and adipose tissue. Stromal tissue shows lymphoplasmacytic infiltrate. A small fragment of a dilated duct lined by a single layer of benign cells is included |
| ‣ Histological grade: | No evidence of malignancy in this biopsy |
| ‣ Mitosis: | |
| ‣ Maximum invasive tumour size: | |
| ‣ Lymph node status: | |
| ‣ Peritumoural lymphovascular invasion: | |
| ‣ DCIS/EIC: | |
| ‣ Margins: | |
| ‣ Pathological stage: | |
| ‣ Biomarkers: | |
| ‣ Comments: | Papillary lesions show intralesional heterogeneity, which explains why the limited sampling achieved with needle core biopsy may miss areas of in situ cancer and foci of invasive cancer. The needle core biopsy is also fragmented because of the cystic nature of the lesion. The patient was referred to a higher centre for MRM and the histopathology report showed an encysted papillary carcinoma |
Case summary:
| Postmenopausal woman presented with a lump in the right breast, diagnosed as complex cystic and solid mass lesion with pleomorphic microcalcifications in right breast, BI-RADS category 5 on imaging, as papillary lesion with atypia on cytology, and as encapsulated papillary carcinoma on histopathology. |
Learning points:
|