



Home / Training / Manuals / Atlas of breast cancer early detection / Cases
Atlas of breast cancer early detection
Filter by language: English / Русский
Go back to the list of case studies
.png) Click on the pictures to magnify and display the legends
Click on the pictures to magnify and display the legends
| Case number: | 059 |
| Age: | 43 |
| Clinical presentation: | Premenopausal woman with average risk of developing breast cancer presented with pain and a lump in the left breast of duration 45 days. Examination revealed a large (6 cm) tender lump with redness of the overlying skin in the upper half of the left breast. |
Mammography:
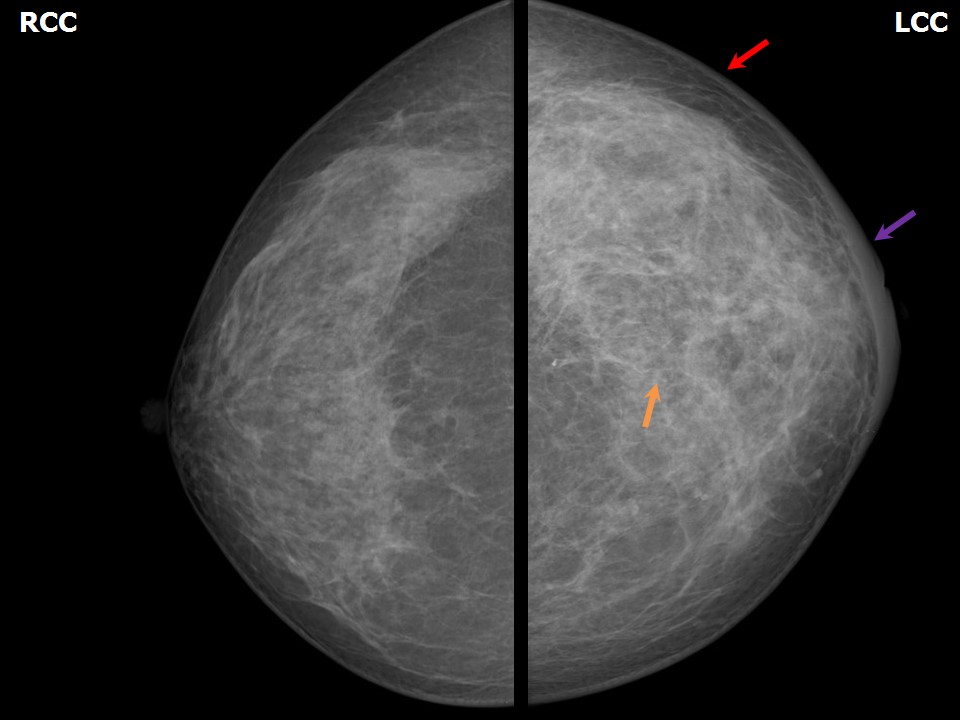 | 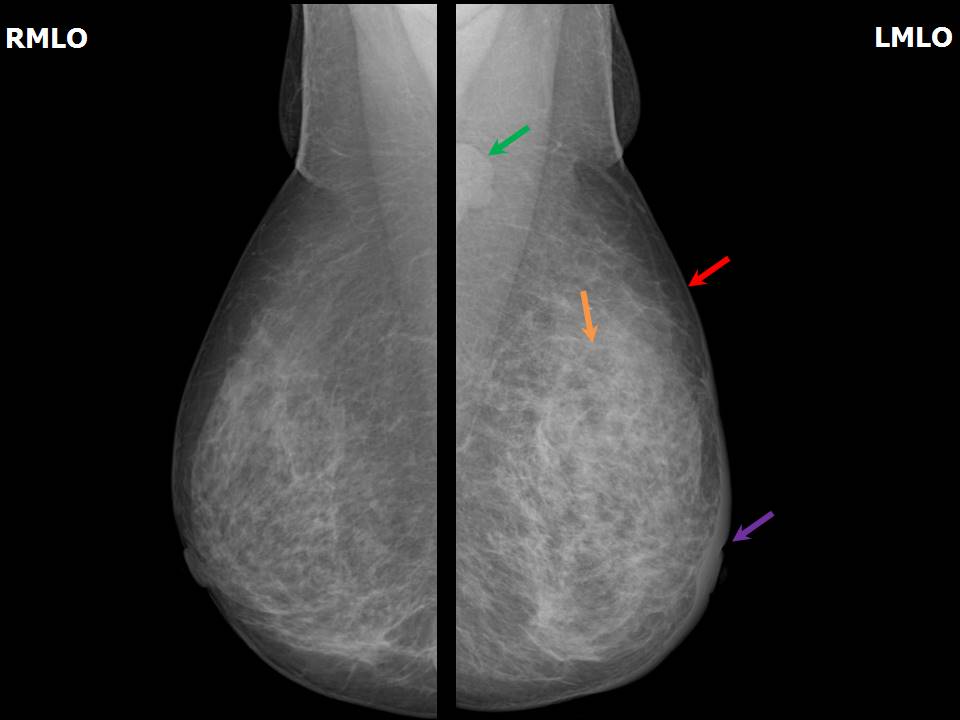 |
| Breast composition: | ACR category c (the breasts are heterogeneously dense, which may obscure small masses) | Mammography features: |
| ‣ Location of the lesion: | Left breast, upper outer quadrant at 24 oclock, middle third |
| ‣ Mass: | |
| • Number: | Obscured by the dense parenchyma |
| • Size: | Not measurable |
| • Shape: | None |
| • Margins: | None |
| • Density: | None |
| ‣ Calcifications: | |
| • Typically benign: | None |
| • Suspicious: | None |
| • Distribution: | None |
| ‣ Architectural distortion: | Present |
| ‣ Asymmetry: | Present with unilateral breast enlargement |
| ‣ Intramammary node: | None |
| ‣ Skin lesion: | None |
| ‣ Solitary dilated duct: | None |
| ‣ Associated features: | Skin thickening, trabecular thickening, axillary lymphadenopathy, architectural distortion, and nipple retraction |
Ultrasound:
 |  |
 |  |
 |
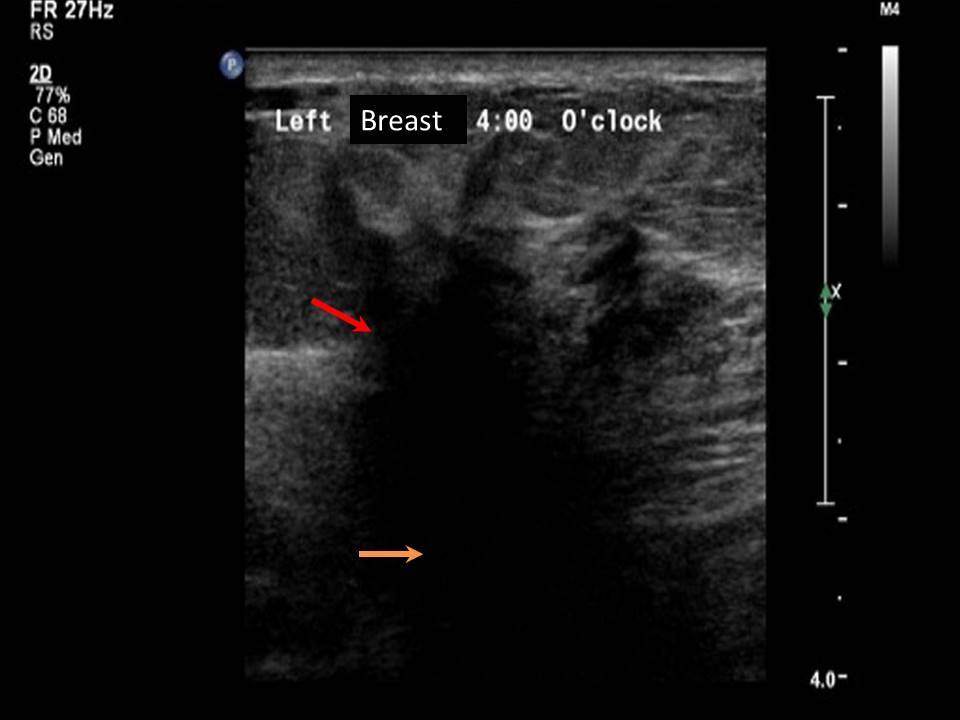
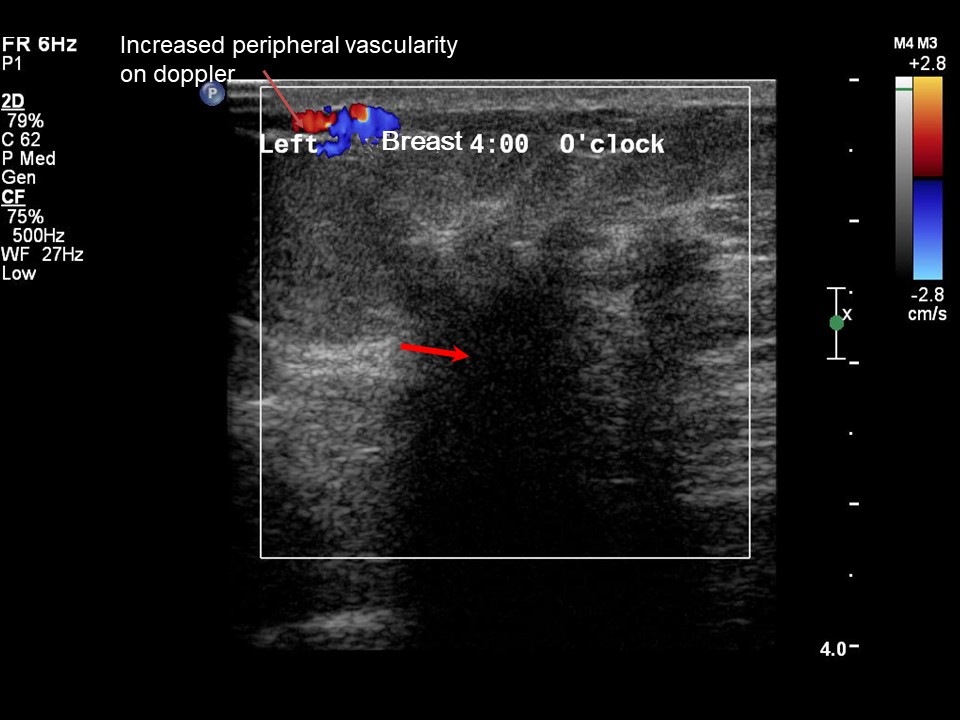
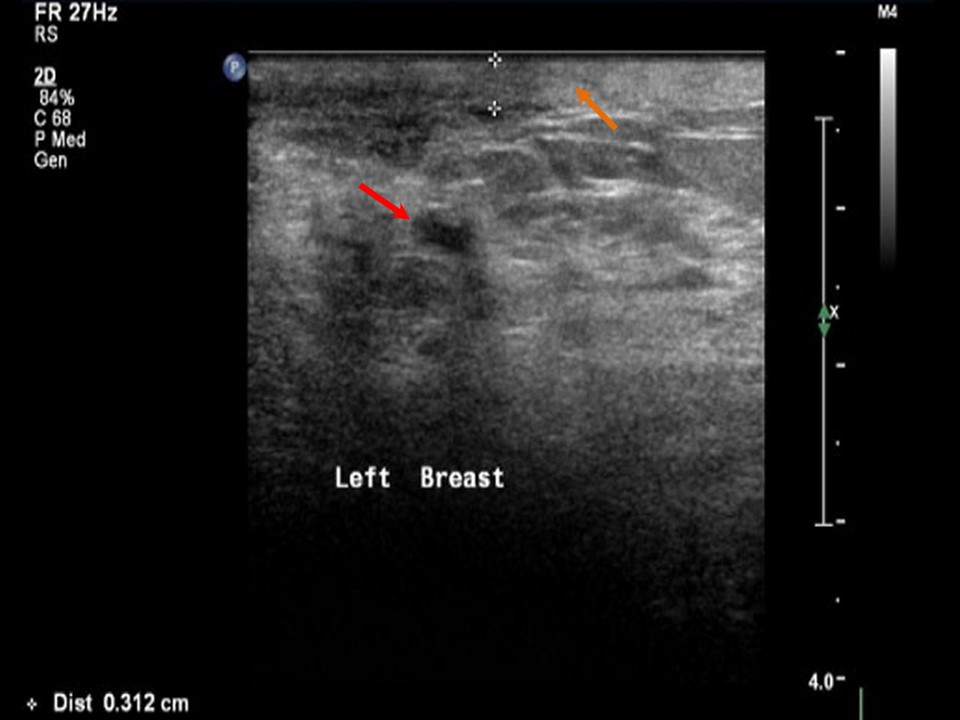
| Ultrasound features: Left breast, outer quadrants at 24 oclock | |
| ‣ Mass | |
| • Location: | Left breast, outer quadrants at 24 oclock |
| • Number: | 1 |
| • Size: | 5.8 × 4.6 cm |
| • Shape: | Irregular |
| • Orientation: | Not parallel |
| • Margins: | Spiculated |
| • Echo pattern: | Hypoechoic |
| • Posterior features: | Strong posterior shadowing |
| ‣ Calcifications: | None |
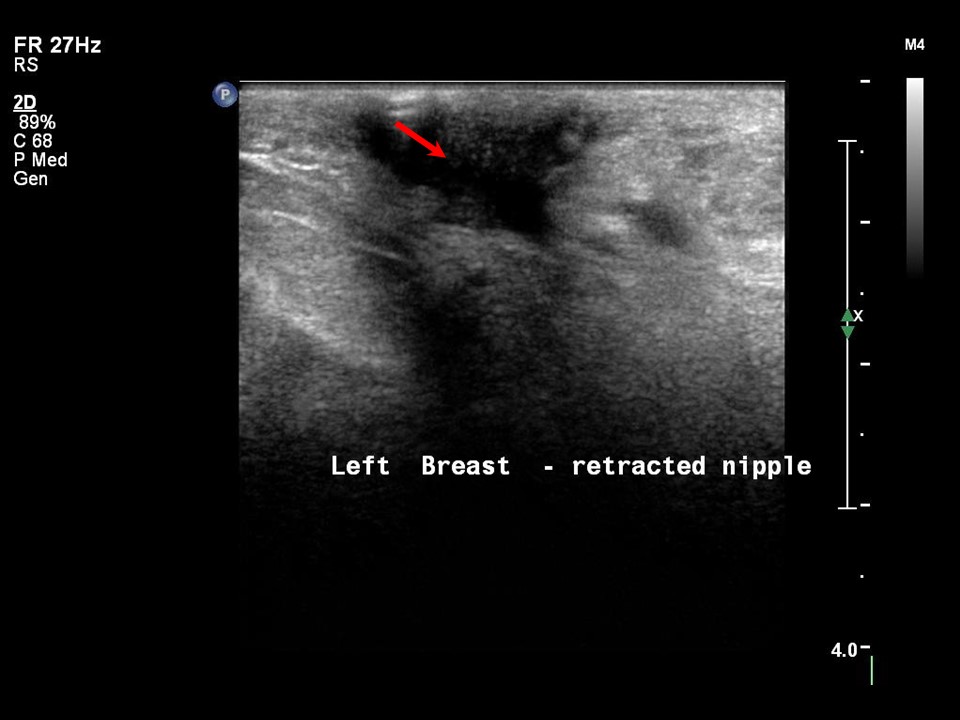
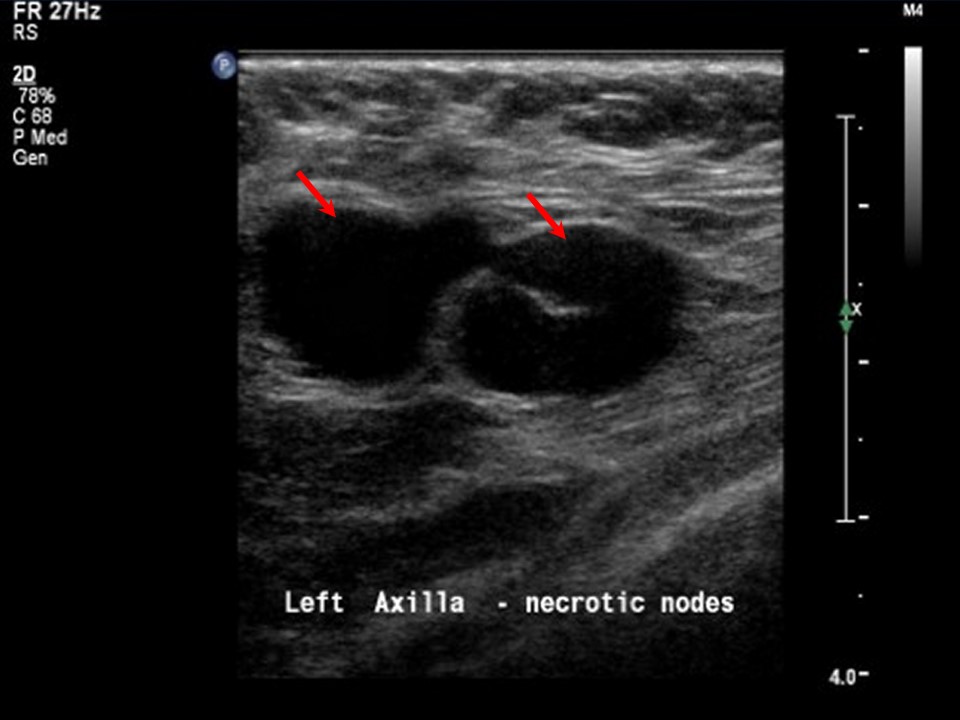
| ‣ Associated features: | Architectural distortion, skin thickening, oedema, internal vascularity, multiple enlarged axillary lymph nodes with loss of central fatty sinus, and nipple retraction |
| ‣ Special cases: | None |
BI-RADS:
BI-RADS Category: 5 (highly suggestive of malignancy)Further assessment:
Further assessment advised: Referral for cytology and for core biopsyCytology:
 |
| Cytology features: | |
| ‣ Type of sample: | FNAC |
| ‣ Site of biopsy: | |
| • Laterality: | Left |
| • Quadrant: | |
| • Localization technique: | Palpation |
| • Nature of aspirate: | whitish |
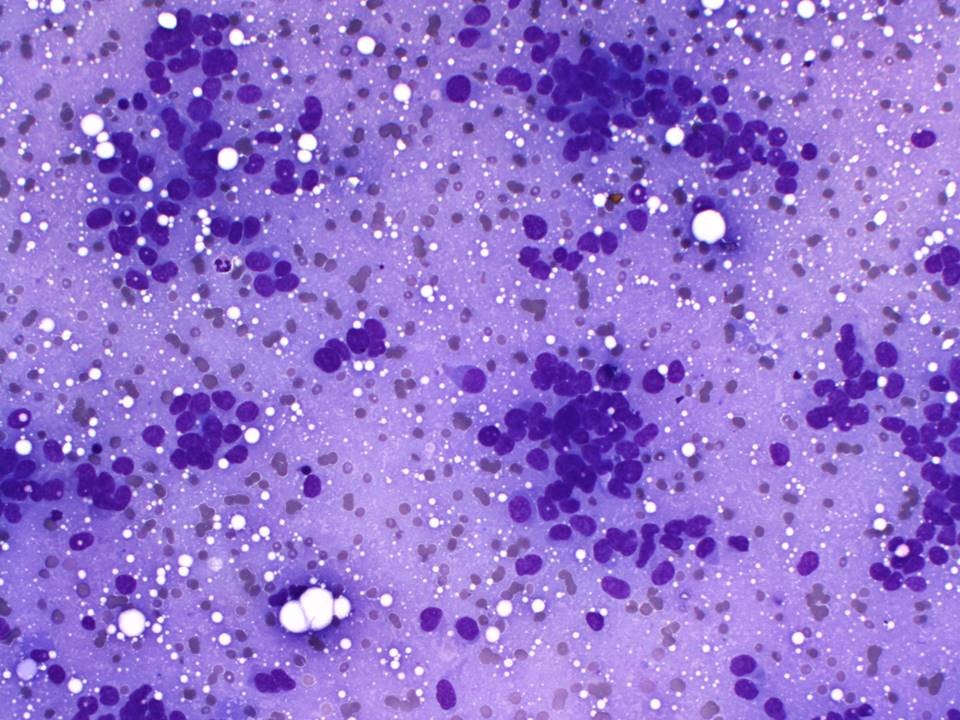
| ‣ Cytological description: | Smears show loosely dispersed malignant cells with mild anisonucleosis. Many single isolated malignant cells are also seen |
| ‣ Reporting category: | Malignant |
| ‣ Diagnosis: | Carcinoma low grade |
| ‣ Comments: | None |
Histopathology:
Core needle biopsy
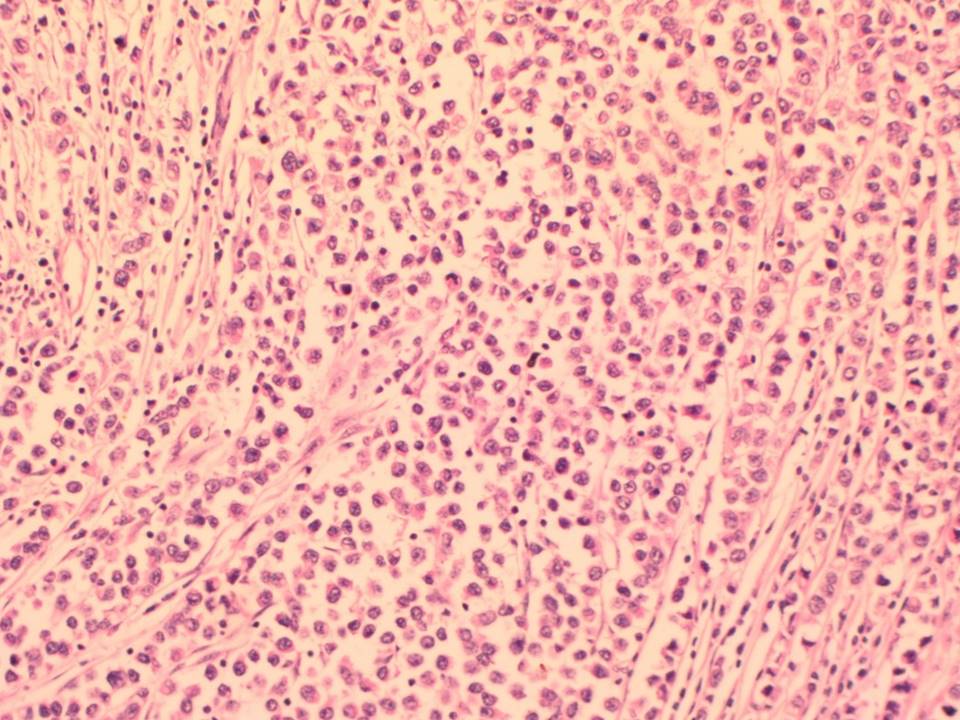 |
| Histopathology features: | |
| ‣ Specimen type: | Core needle biopsy |
| ‣ Laterality: | Left |
| ‣ Macroscopy: | Three firm whitish core tissue bits, each 20 mm in length |
| ‣ Histological type: | Sections shows features of breast carcinoma with a lobular pattern of infiltration in the biopsy specimen. Malignancy is present in 30% of the core biopsy tissue. Normal ducts are also seen in the section |
| ‣ Histological grade: | |
| ‣ Mitosis: | |
| ‣ Maximum invasive tumour size: | |
| ‣ Lymph node status: | |
| ‣ Peritumoural lymphovascular invasion: | |
| ‣ DCIS/EIC: | |
| ‣ Margins: | |
| ‣ Pathological stage: | |
| ‣ Biomarkers: | |
| ‣ Comments: |
Case summary:
| Premenopausal woman presented with painful left breast lump. Diagnosed as inflammatory left breast carcinoma with breast oedema, skin thickening, and left nipple retraction, BI-RADS 5 on imaging, as breast carcinoma on cytology, and as invasive lobular carcinoma on histopathology of needle core biopsy. |
Learning points:
|