



Home / Training / Manuals / Atlas of breast cancer early detection / Cases
Atlas of breast cancer early detection
Filter by language: English / Русский
Go back to the list of case studies
.png) Click on the pictures to magnify and display the legends
Click on the pictures to magnify and display the legends
| Case number: | 122 |
| Age: | 68 |
| Clinical presentation: | Postmenopausal woman with increased risk of developing breast cancer because of a family history of breast cancer presented with excoriation of the left nipple with minimal serous nipple discharge. Examination did not reveal any lumps in the breast. |
 |
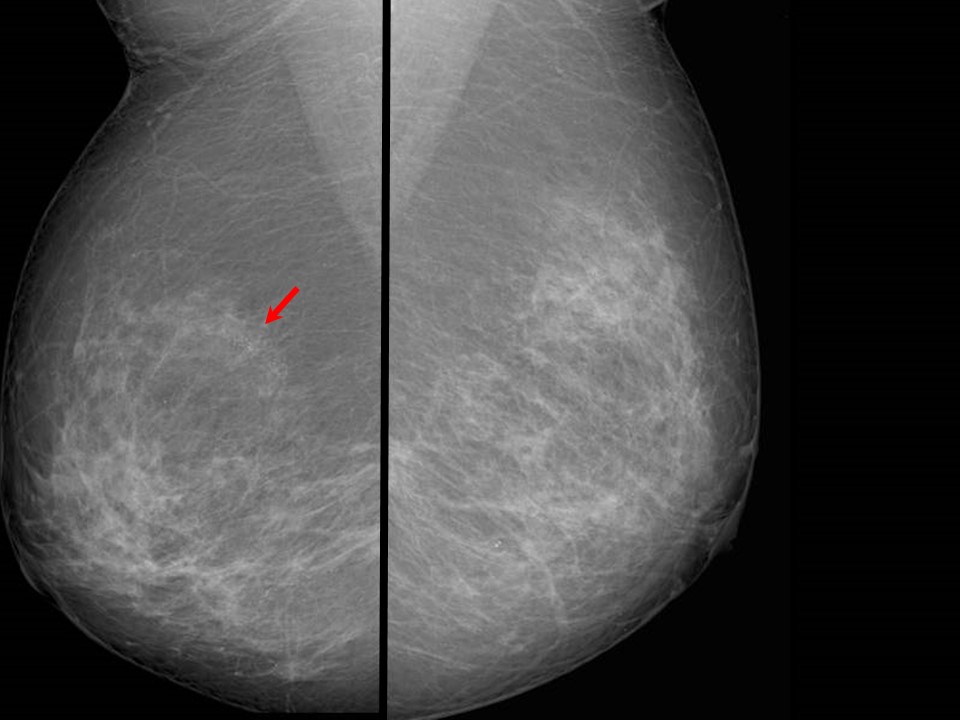
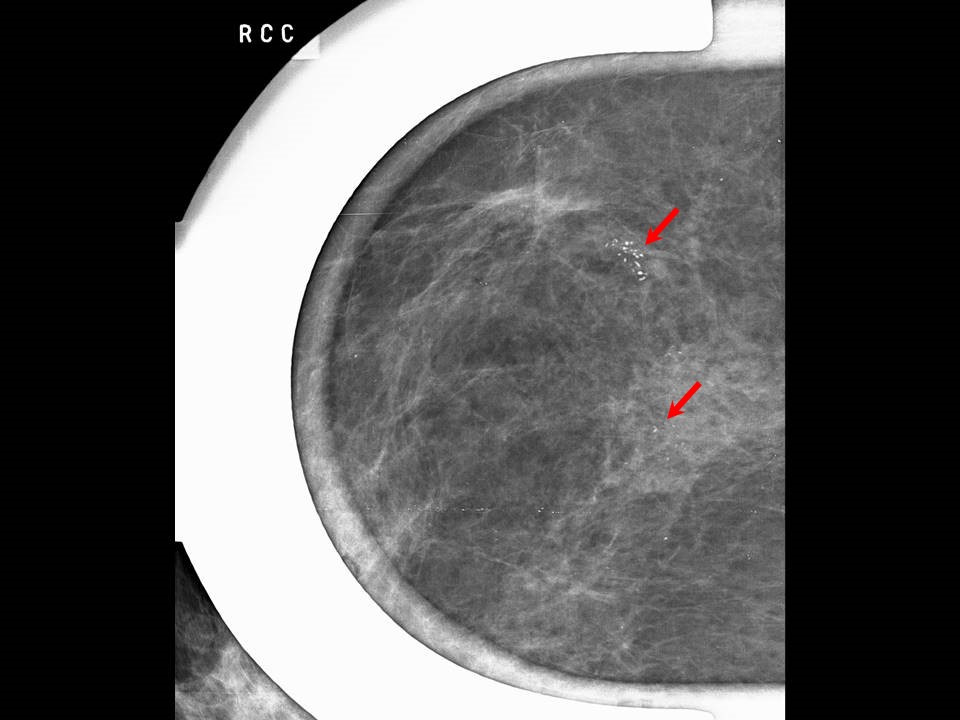
Mammography:
 |  |
 |
| Breast composition: | ACR category b (there are scattered areas of fibroglandular density) | Mammography features: |
| ‣ Location of the lesion: | Left breast, central portion of the breast, central zone, anterior third |
| ‣ Mass: | |
| • Number: | 1 |
| • Size: | 0.4 cm in greatest dimension |
| • Shape: | Irregular |
| • Margins: | Indistinct |
| • Density: | Equal |
| ‣ Calcifications: | |
| • Typically benign: | None |
| • Suspicious: | None |
| • Distribution: | None |
| ‣ Architectural distortion: | None |
| ‣ Asymmetry: | None |
| ‣ Intramammary node: | None |
| ‣ Skin lesion: | None |
| ‣ Solitary dilated duct: | None |
| ‣ Associated features: | Nipple changes |
| Mammography features: | |
| ‣ Location of the lesion: | Right breast, upper outer quadrant at 10 oclock, middle third and right breast, lower inner quadrant at 5 oclock, middle third |
| ‣ Mass: | |
| • Number: | 0 |
| • Size: | None |
| • Shape: | None |
| • Margins: | None |
| • Density: | None |
| ‣ Calcifications: | |
| • Typically benign: | None |
| • Suspicious: | Fine pleomorphic |
| • Distribution: | Grouped |
| ‣ Architectural distortion: | Focal |
| ‣ Asymmetry: | None |
| ‣ Intramammary node: | None |
| ‣ Skin lesion: | None |
| ‣ Solitary dilated duct: | None |
| ‣ Associated features: | Architectural distortion and calcifications pleomorphic in three groups |
Ultrasound:
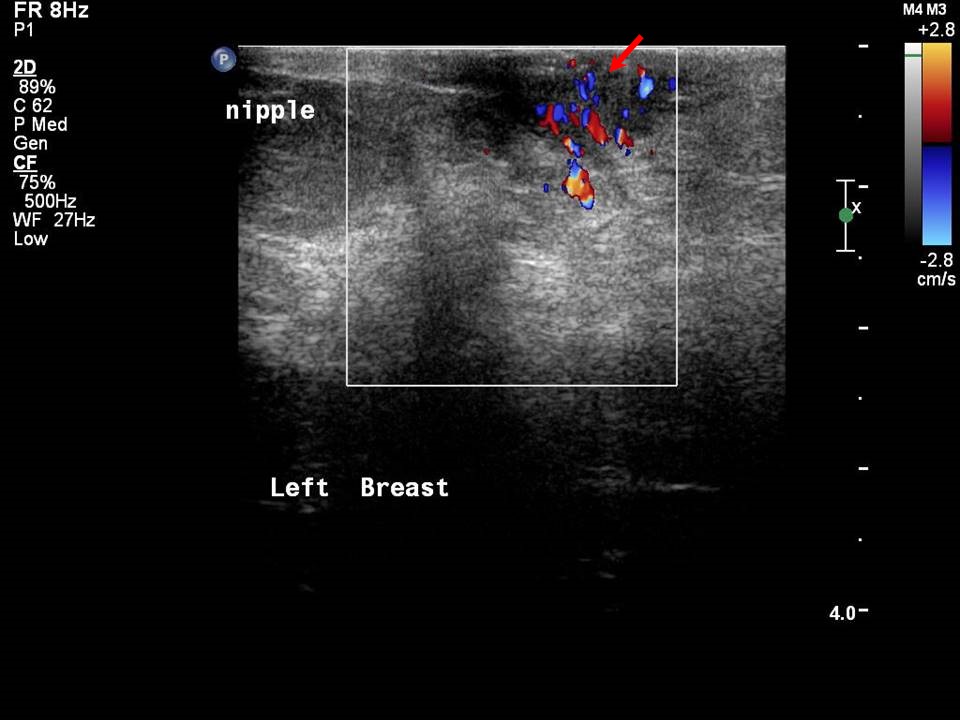 | 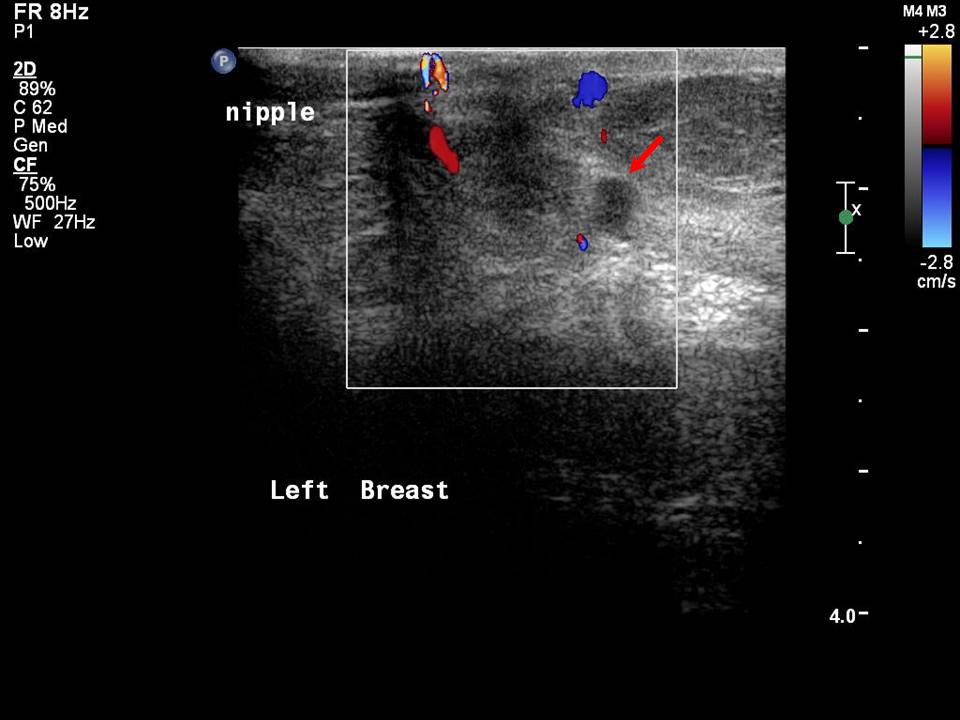 |
| Ultrasound features: Left breast, central portion of the breast | |
| ‣ Mass | |
| • Location: | Left breast, central portion of the breast |
| • Number: | 1 |
| • Size: | 0.4 cm in greatest dimension |
| • Shape: | Oval |
| • Orientation: | Not parallel |
| • Margins: | Indistinct |
| • Echo pattern: | Hypoechoic |
| • Posterior features: | No posterior features |
| ‣ Calcifications: | None |
| ‣ Associated features: | Nipple changes and increased vascularity |
| ‣ Special cases: | None |
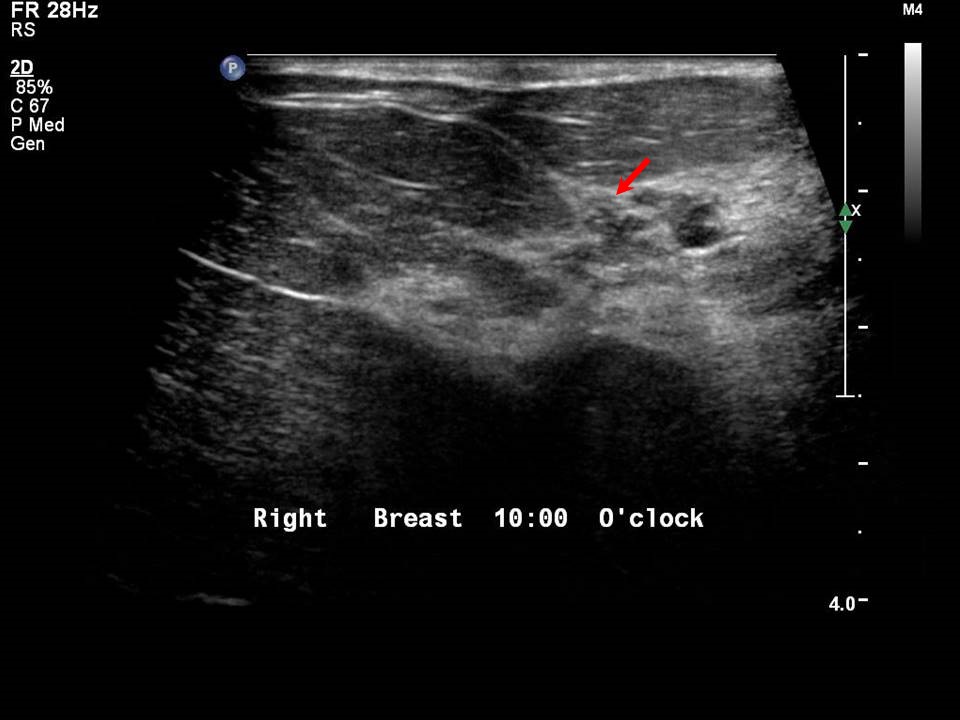 |
| Ultrasound features: Right breast, upper outer quadrant at 10-11 o'clock | |
| ‣ Mass | |
| • Location: | Right breast, upper outer quadrant at 10-11 o'clock |
| • Number: | 0 |
| • Size: | None |
| • Shape: | None |
| • Orientation: | None |
| • Margins: | None |
| • Echo pattern: | None |
| • Posterior features: | No posterior features |
| ‣ Calcifications: | None |
| ‣ Associated features: | Architectural distortion in right breast upper outer quadrant at 1011 oclock |
| ‣ Special cases: | None |
BI-RADS:
BI-RADS Category (bilateral): 4C (high suspicion for malignancy)Further assessment:
Further assessment advised: Further imaging with breast MRIMRI:
 |
| MRI features: | ||
| ‣ MRI features: | Amount of fibroglandular tissue: ACR category b (scattered fibroglandular tissue). Background parenchymal enhancement: Moderate (2550%), symmetrical | |
| ‣ Location: | Left breast | |
| ‣ Focus: | No | |
| ‣ Mass: | ||
| • Shape: | No | |
| • Margin: | No | |
| • Internal enhancement: | No | |
| • Kinetic curve: | No | |
| ‣ Non-mass enhancement: | ||
| • Distribution: | Left nippleareolar complex | |
| • Internal enhancement: | Early enhancement followed by plateau in left nippleareolar complex, extending to retroareolar region | |
| ‣ Non-enhancing findings: | No | |
| ‣ Associated features: | No | |
| ‣ Axillary nodes: | No | |
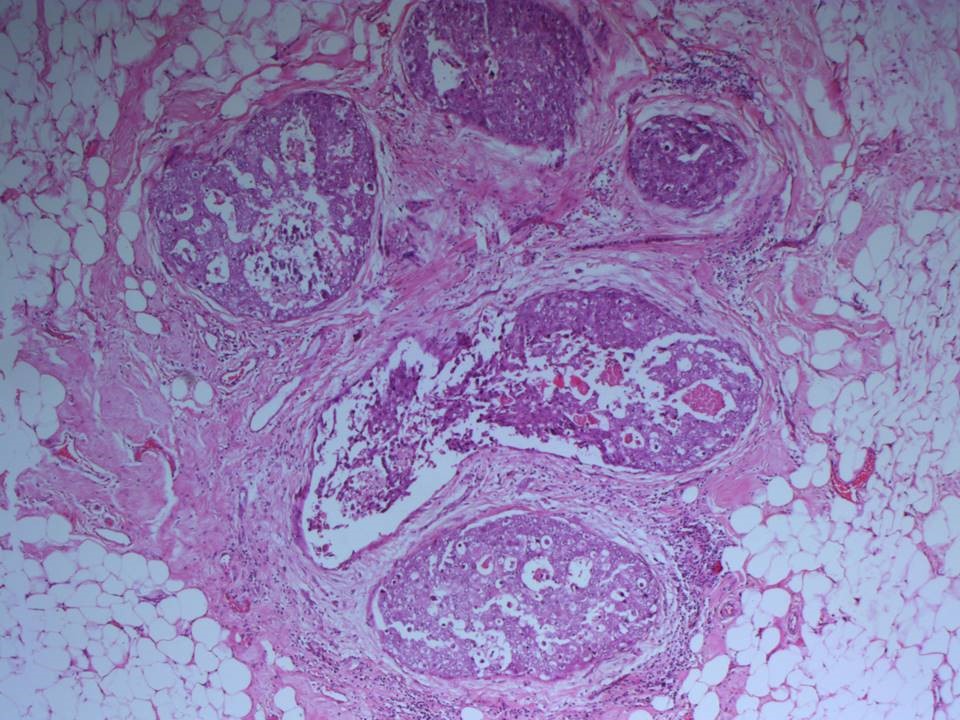
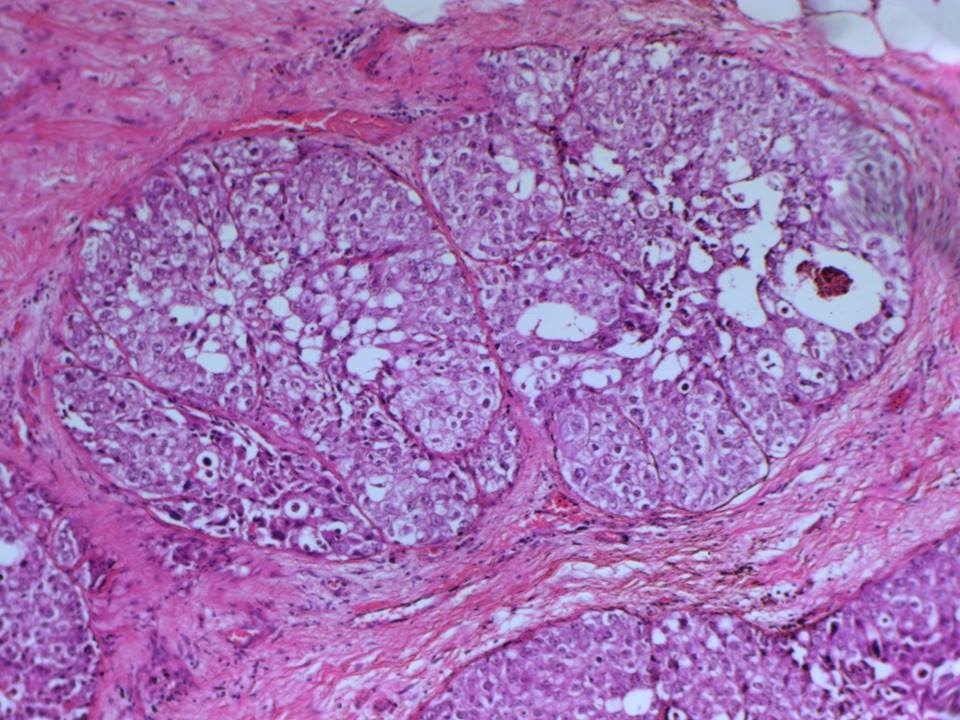
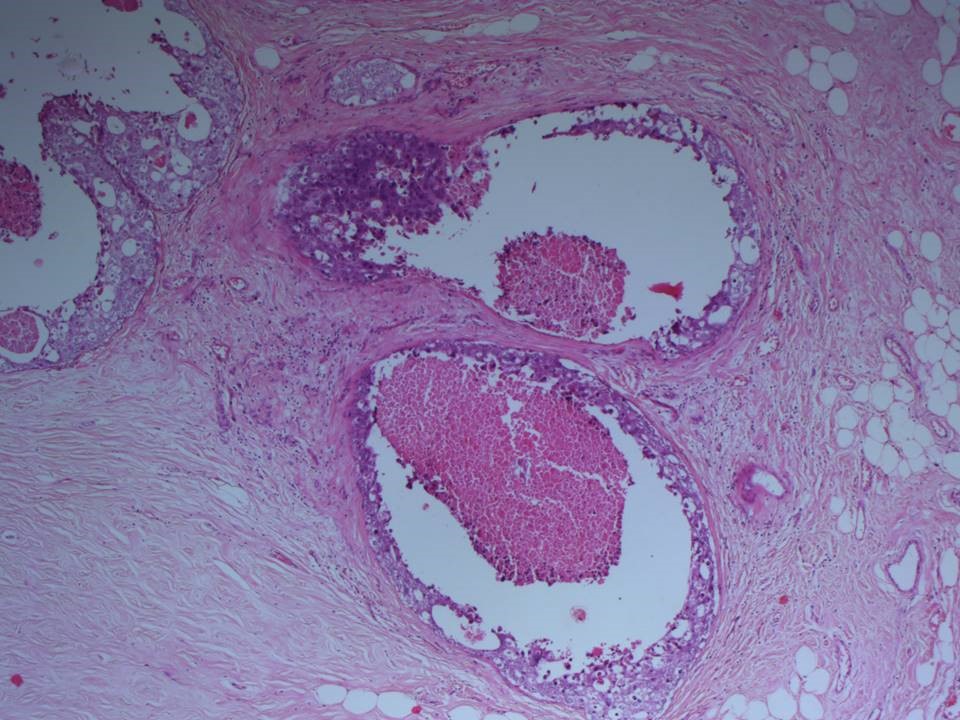
Histopathology:
Right breast, wire-localized excision biopsy, September 2016
 |
| Histopathology features: | |
| ‣ Specimen type: | Right breast, wire-localized excision biopsy, September 2016 |
| ‣ Laterality: | Right |
| ‣ Macroscopy: | Right breast lumpectomy specimen (8.5 × 4.2 × 1.3 cm) oriented with long suture laterally and short suture superiorly. On serial sectioning, a diffuse firm whitish lesion (approximately 2.2 × 0.8 × 0.6 cm) is identified. It is located 0.3 cm from the anterior margin, 2.5 cm from the posterior margin, 1.5 cm from the superior margin, 2.0 cm from the inferior margin, 0.5 cm from the medial margin, and 2.8 cm from the lateral margin. The remaining breast parenchyma is unremarkable |
| ‣ Histological type: | Multiple sections reveal no invasive tumour |
| ‣ Histological grade: | |
| ‣ Mitosis: | |
| ‣ Maximum invasive tumour size: | |
| ‣ Lymph node status: | |
| ‣ Peritumoural lymphovascular invasion: | Not seen |
| ‣ DCIS/EIC: | DCIS of solid type, high nuclear grade with comedo necrosis. Calcification is seen within DCIS |
| ‣ Margins: | All other margins free of DCIS |
| ‣ Pathological stage: | Van Nuys Prognostic index is 9 |
| ‣ Biomarkers: | ER negative, PR negative, and HER2 positive (score 3) |
| ‣ Comments: | No foci of invasion identified. The adjacent breast shows fibrocystic changes in the form of UDH and apocrine metaplasia |
Right breast, MRM (post lumpectomy), November 2016
 |
| Histopathology features: | |
| ‣ Specimen type: | Right breast, MRM (post lumpectomy), November 2016 |
| ‣ Laterality: | Right |
| ‣ Macroscopy: | Specimen (19.0 × 18.0 × 8.5 cm) with overlying skin flap (19.5 × 13.0 cm). The nipple and areola are retracted. A linear scar (4.0 × 0.2 cm) is located in the upper outer quadrant, 8 cm from the nipple. On serial sectioning, a cavitary lesion (6.0 × 4.0 × 3.5 cm) with yellowish ragged walls is identified below the scar in the upper outer quadrant. It is abutting the skin with scar and 2.0 cm from the base. The remaining breast tissue is unremarkable |
| ‣ Histological type: | Invasive tumour is not seen |
| ‣ Histological grade: | |
| ‣ Mitosis: | |
| ‣ Maximum invasive tumour size: | |
| ‣ Lymph node status: | 0/2 |
| ‣ Peritumoural lymphovascular invasion: | |
| ‣ DCIS/EIC: | DCIS of solid type, high nuclear grade without necrosis. EIC is absent |
| ‣ Margins: | Paget disease of the nipple is not seen. The base is free of tumour. Overlying skin with scar is unremarkable |
| ‣ Pathological stage: | |
| ‣ Biomarkers: | |
| ‣ Comments: | The adjacent breast shows fibrocystic changes, extensive columnar cell alteration, and calcification |
Left breast, lumpectomy, November 2016
 | 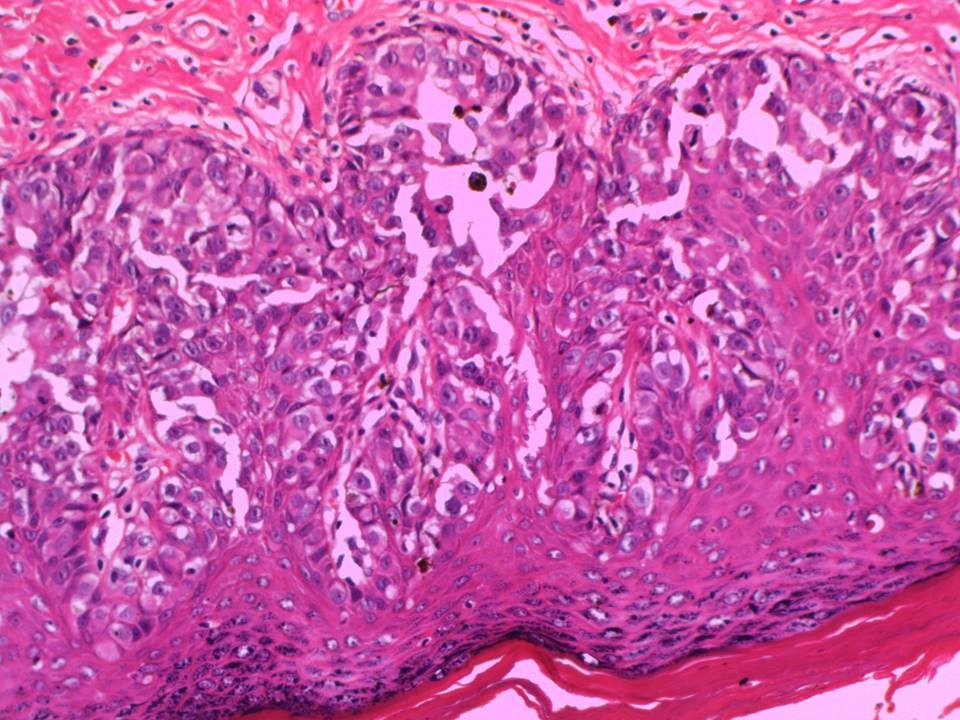 |
| Histopathology features: | |
| ‣ Specimen type: | Left breast, lumpectomy, November 2016 |
| ‣ Laterality: | Left |
| ‣ Macroscopy: | Left breast lumpectomy specimen (6.0 × 5.5 × 2.5 cm) oriented with long suture laterally and short suture superiorly. The overlying skin flap with nipple areola measures 3.5 × 2.5 cm. The nipple is ulcerated. On serial sectioning, a firm whitish diffuse lesion is identified (1.5 × 1.2 × 1.0 cm) at the nipple. The nipple lesion is submitted entirely. It is located 4.5 cm from the posterior margin, 0.9 cm from the superior margin, 0.5 cm from the inferior margin, 2.0 cm from the medial margin, and 3.5 cm from the lateral margin. The remaining breast parenchyma is unremarkable |
| ‣ Histological type: | Multiple sections reveal no invasive tumour |
| ‣ Histological grade: | |
| ‣ Mitosis: | |
| ‣ Maximum invasive tumour size: | |
| ‣ Lymph node status: | 0/7 |
| ‣ Peritumoural lymphovascular invasion: | Not seen |
| ‣ DCIS/EIC: | DCIS of comedo type, high nuclear grade with necrosis. EIC is absent |
| ‣ Margins: | Paget disease of nipple and areola is present. Lateral cut margin shows a single duct with DCIS 2 mm from the inked surface |
| ‣ Pathological stage: | |
| ‣ Biomarkers: | |
| ‣ Comments: |
Case summary:
| Postmenopausal woman with high risk of developing breast cancer presented with excoriation of the left nipple with minimal serous nipple discharge. Examination did not reveal any lump in the breast. Diagnosed as right breast suspicious grouped microcalcifications and left nipple suspicious increased vascularity, BI-RADS category 4C, bilateral synchronous on imaging. DCIS, high grade seen bilaterally with Paget disease on left side on histopathology. |
Learning points:
|