



Home / Training / Manuals / Atlas of breast cancer early detection / Learning
.png)
Click on the pictures to magnify and display the legends

Click on this icon to display a case study
Atlas of breast cancer early detection
Filter by language: English / РусскийBreast pathology Histopathology of the breast Specimen grossing |
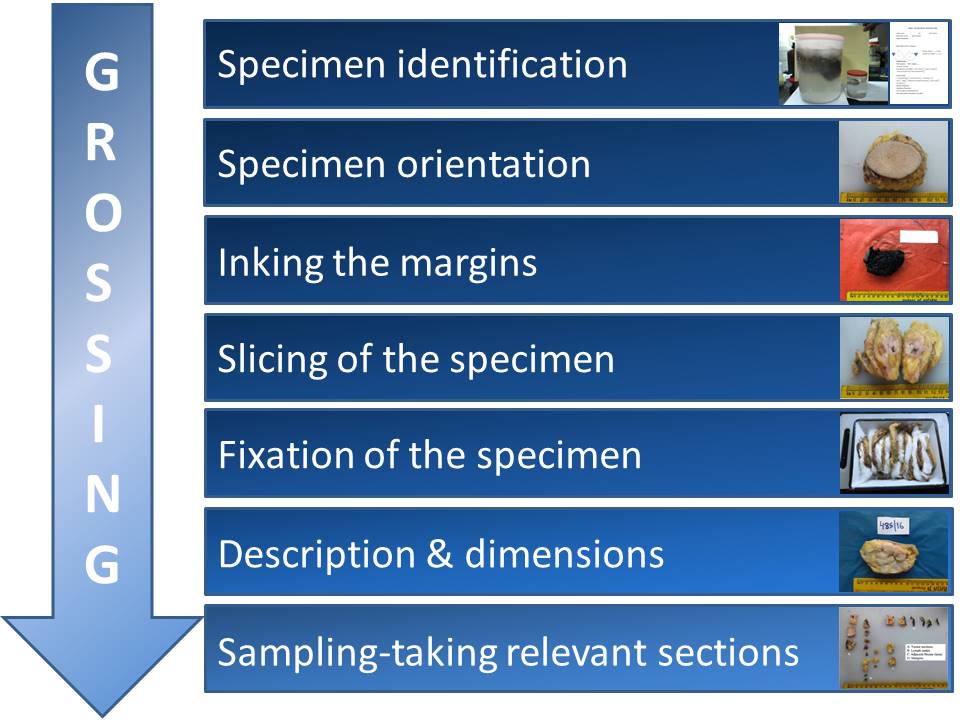
In specimen grossing, the received specimen is thoroughly inspected, measured, and described. Diagnostically valuable sections are taken as appropriate.
The objectives of grossing are:
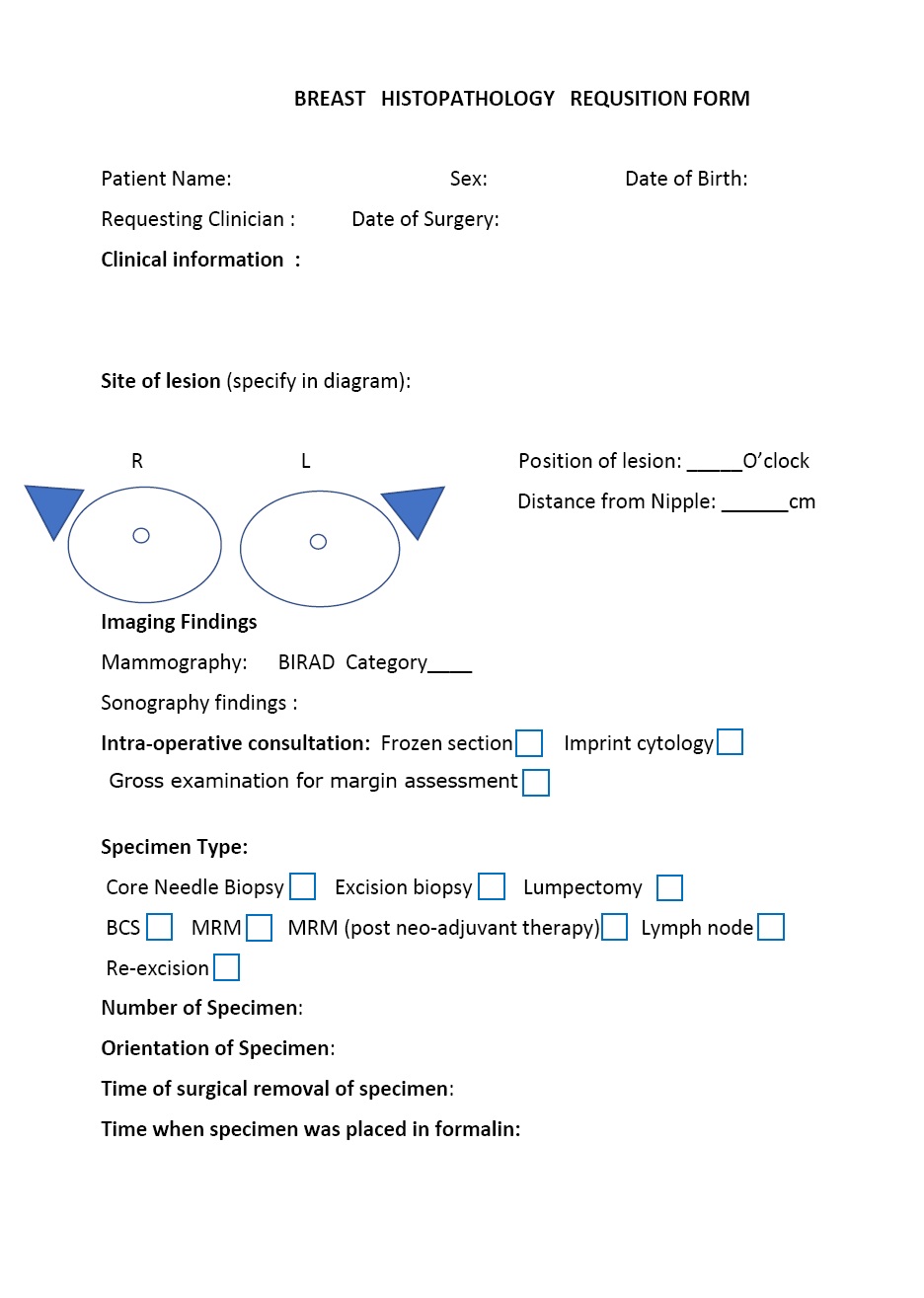
Preparation Before proceeding with grossing of the specimen, it is important to:
Specimen identification
Specimen orientation
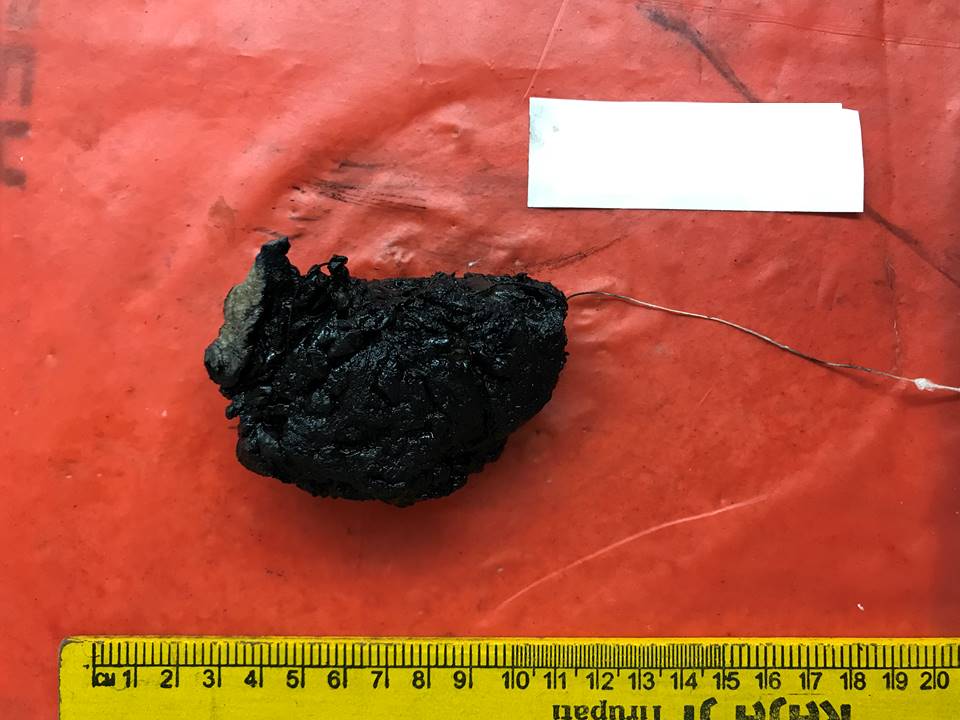
Inking the margins The margins are inked to identify the surgical plane of excision microscopically. Any washproof ink, such as India ink or fabric paint, can be used.
Slicing of the specimen Specimens are sliced to facilitate fixation.
Fixation of the specimen
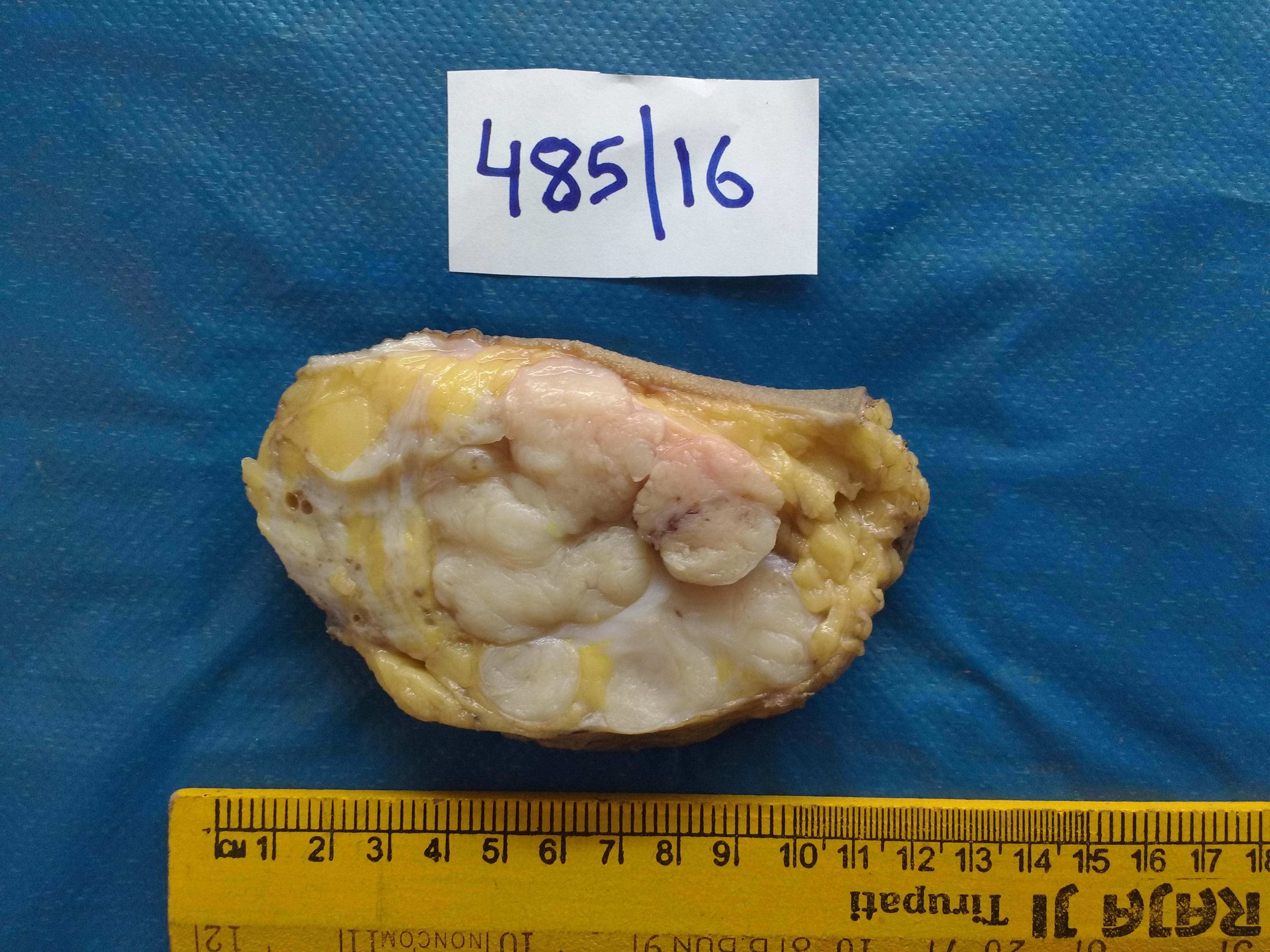
Measuring the dimensions of the specimen
Grossing of the axillary lymph nodes
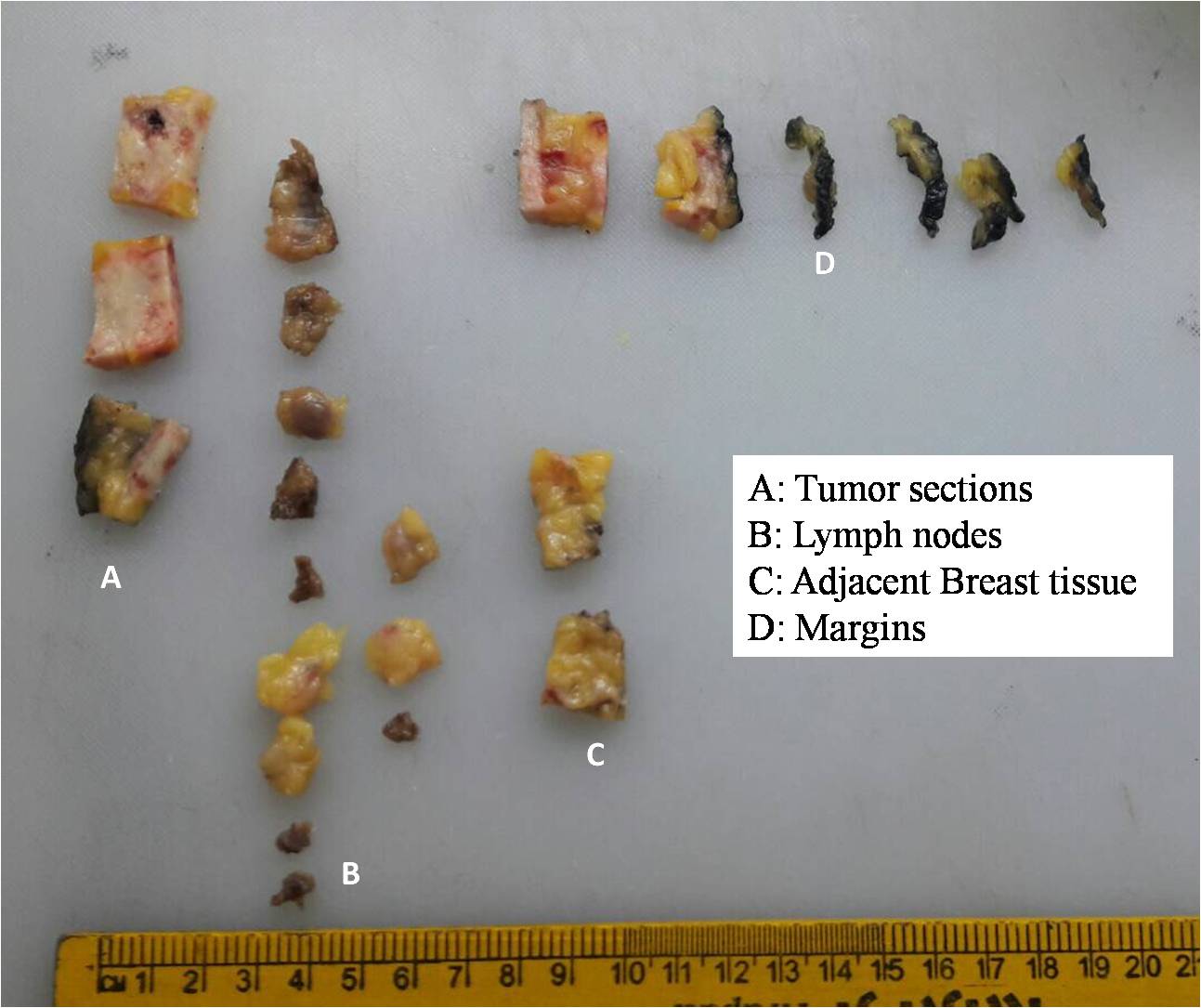
Sampling
The sections to be submitted after grossing of a radical mastectomy specimen After grossing of a radical mastectomy specimen, the following sections should be submitted:
The sections to be submitted after grossing of a breast-conserving surgery specimen After grossing of a specimen from breast-conserving surgery, the following sections should be submitted: |










Click on the pictures to magnify and display the legends
Click on this icon to display a case study
25 avenue Tony Garnier CS 90627 69366, LYON CEDEX 07 France - Tel: +33 (0)4 72 73 84 85
© IARC 2026 - Terms of use - Privacy Policy.
© IARC 2026 - Terms of use - Privacy Policy.