



Learning colposcopy
Colposcopic appearance of normal cervix
The colposcopic examination
Detection of infections & benign conditions of cervix
Detection of cervical neoplasias
Treatment of cervical intraepithelial neoplasia
Treatment by cryotherapy
Treatment by thermal ablation
Treatment by LLETZ (LEEP)
Treatment by cold-knife conization (CKC)
Cases
Normal
Squamous metaplasia and ectropion
Inflammation and cervicitis
Low grade
High grade
Early and advanced cancers
Miscellaneous
Post treatment
Search with IFCPC criteria
Search with Swede score criteria
Quiz Foreword
Acknowledgement
Authors
Suggested citation
Home
Atlas of Colposcopy: Principles and Practice
Filter by language: English / 中文 / Français / Español / Português / Русский| DETECTION OF CERVICAL NEOPLASIAS |
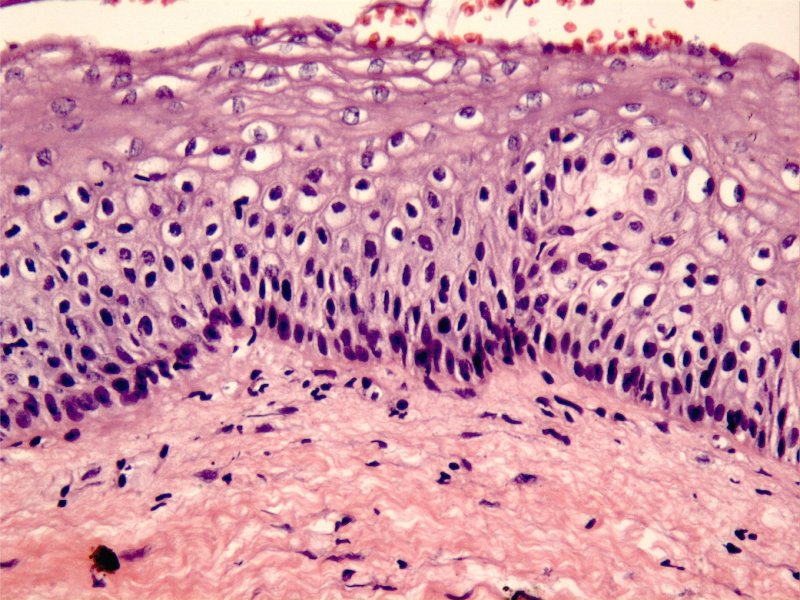
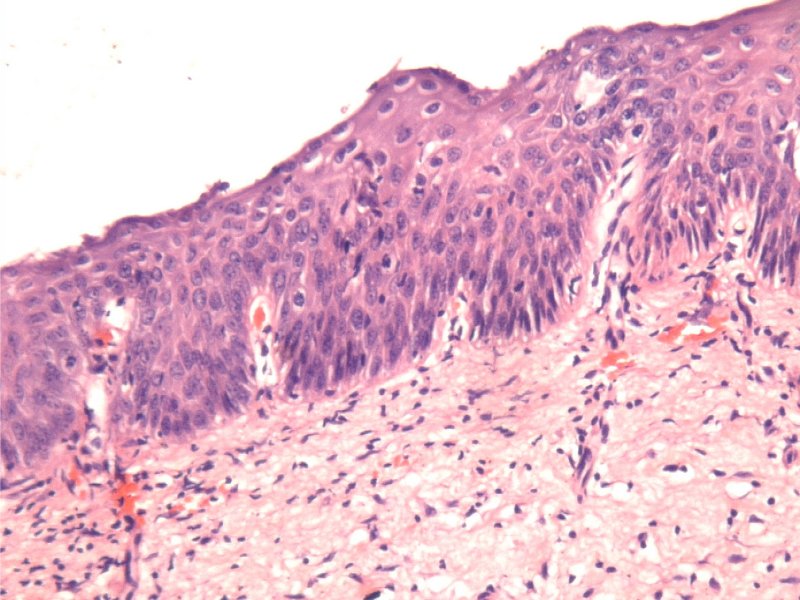
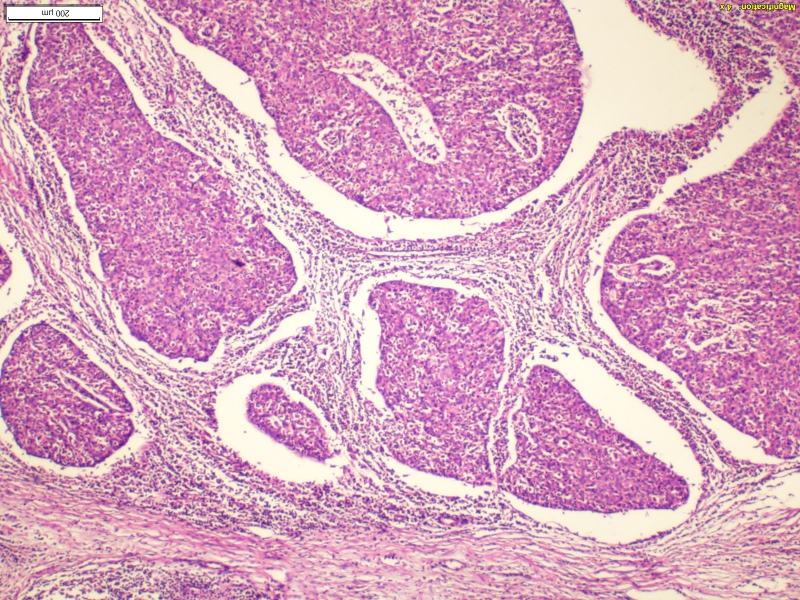
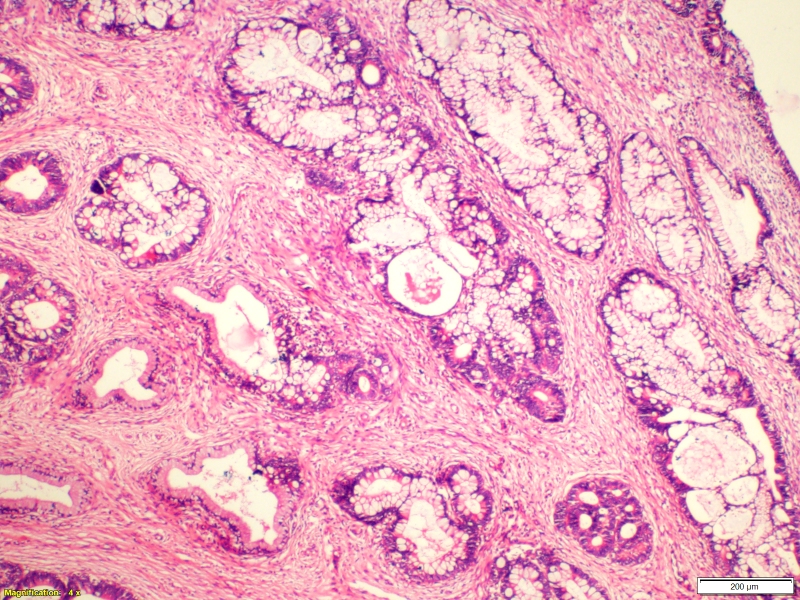
Cervical cancer is a very rare long-term outcome of persistent infection with high-risk human papillomavirus (HPV). To begin with, HPV infection leads to premalignant changes that are histopathologically characterized by undifferentiated cells occupying varying levels of the cervical epithelium. The undifferentiated cells are associated with nuclear abnormalities such as enlarged nuclei, hyperchromasia, nuclear polymorphism, and also mitotic bodies. Depending on the thickness of the epithelium occupied by the undifferentiated cells and the degree of nuclear abnormality, the premalignant lesions (also known as cervical intraepithelial neoplasia, CIN) are classified as CIN1 (lower third of the epithelium involved), CIN2 (lower two thirds of the epithelium involved), and CIN3 (more than lower two thirds or entire thickness of the epithelium involved). CIN1 is the result of transient HPV infection and rarely progresses. CIN1 is also categorized as low-grade squamous intraepithelial lesion (LSIL). CIN3 is the true cervical cancer precursor, with a very high risk of progression to invasive cancer. CIN2 is of intermediate risk between CIN1 and CIN3. CIN2 and CIN3 are jointly categorized as high-grade squamous intraepithelial lesion (HSIL). The basement membrane of the epithelium remains intact in LSIL or HSIL, and the undifferentiated cells remain confined to the epithelium. If the undifferentiated cells breach the basement membrane and spread beyond the epithelium, the disease becomes invasive cancer. The majority of cervical cancers arise from squamous cells and are called squamous cell carcinoma. Malignancies arising from glandular cells are known as adenocarcinoma. |
25 avenue Tony Garnier CS 90627 69366, LYON CEDEX 07 France - Tel: +33 (0)4 72 73 84 85
© IARC 2024 - Terms of use - Privacy Policy.
© IARC 2024 - Terms of use - Privacy Policy.