



Learning colposcopy
Colposcopic appearance of normal cervix
The colposcopic examination
Detection of infections & benign conditions of cervix
Detection of cervical neoplasias
Treatment of cervical intraepithelial neoplasia
Treatment by cryotherapy
Treatment by thermal ablation
Treatment by LLETZ (LEEP)
Treatment by cold-knife conization (CKC)
Cases
Normal
Squamous metaplasia and ectropion
Inflammation and cervicitis
Low grade
High grade
Early and advanced cancers
Miscellaneous
Post treatment
Search with IFCPC criteria
Search with Swede score criteria
Quiz Foreword
Acknowledgement
Authors
Suggested citation
Home
Atlas of Colposcopy: Principles and Practice
Filter by language: English / 中文 / Français / Español / Português / Русский| Diagnosing adenocarcinoma in situ (AIS) and adenocarcinoma |
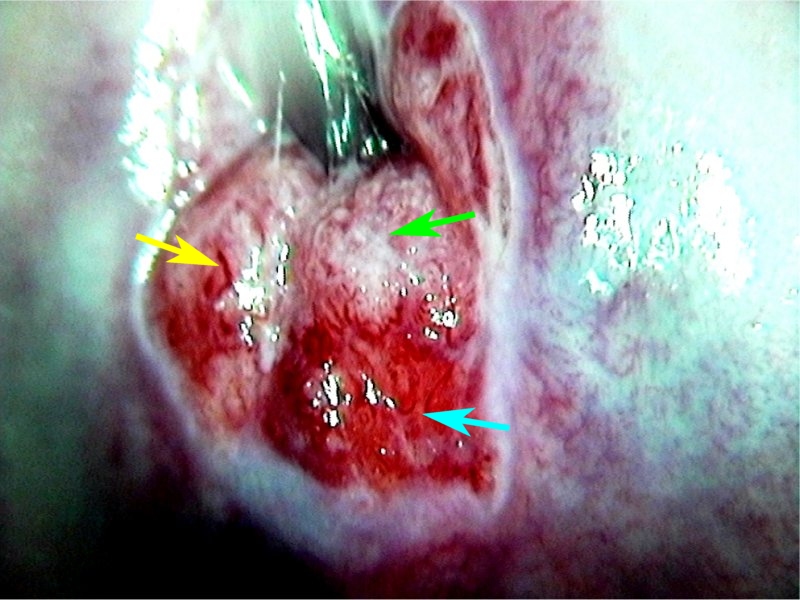
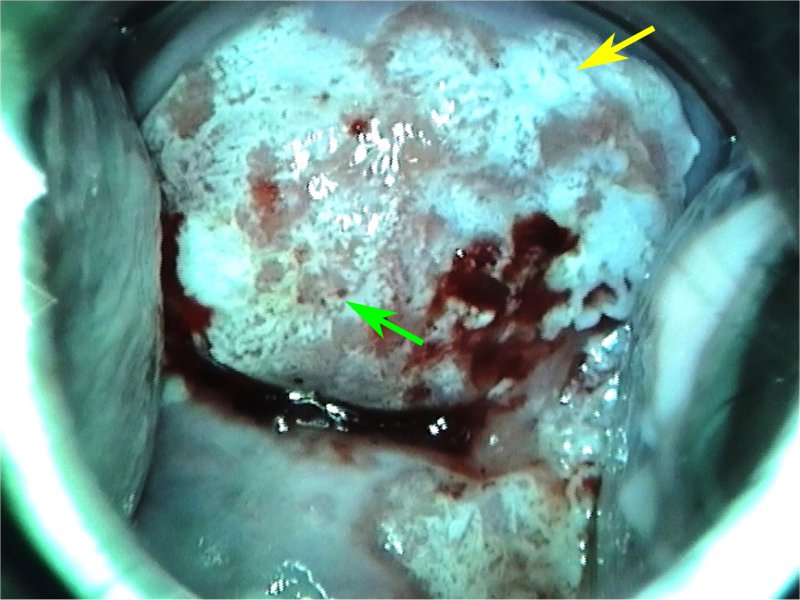
Normal columnar epithelium becomes temporarily white after application of acetic acid. If the acetowhiteness persists and is dense in intensity, glandular lesions should be suspected. The lesion extends into the endocervical canal. There may be abnormal blood vessels on the lesion. The villi of the columnar epithelium become fused to each other. In adenocarcinoma in situ (AIS) or adenocarcinoma, multiple dense acetowhite areas are typically seen on the columnar epithelium. The columnar epithelium appears as if grated coconut has been sprinkled on it. Adenocarcinoma is suspected if the dense acetowhite area is on the columnar epithelium, has an irregular surface, and has abnormal blood vessels. The atypical blood vessels of adenocarcinoma are often parallel to each other. However, it is important to note that it is difficult to perform colposcopy of the endocervix. If the cytology suggests a glandular lesion, an endocervical curettage from all 4 sides of the endocervix should be done even if there is no visible lesion. If the HPV test is positive and cytology suggests a glandular lesion, a LLETZ procedure or cone biopsy will need to be performed.
|

25 avenue Tony Garnier CS 90627 69366, LYON CEDEX 07 France - Tel: +33 (0)4 72 73 84 85
© IARC 2025 - Terms of use - Privacy Policy.
© IARC 2025 - Terms of use - Privacy Policy.