



Learning colposcopy
Colposcopic appearance of normal cervix
The colposcopic examination
Detection of infections & benign conditions of cervix
Detection of cervical neoplasias
Treatment of cervical intraepithelial neoplasia
Treatment by cryotherapy
Treatment by thermal ablation
Treatment by LLETZ (LEEP)
Treatment by cold-knife conization (CKC)
Cases
Normal
Squamous metaplasia and ectropion
Inflammation and cervicitis
Low grade
High grade
Early and advanced cancers
Miscellaneous
Post treatment
Search with IFCPC criteria
Search with Swede score criteria
Quiz Foreword
Acknowledgement
Authors
Suggested citation
Home
Atlas of Colposcopy: Principles and Practice
Filter by language: English / 中文 / Français / Español / Português / Русский| Condyloma and subclinical papillomavirus infection (SPI) |
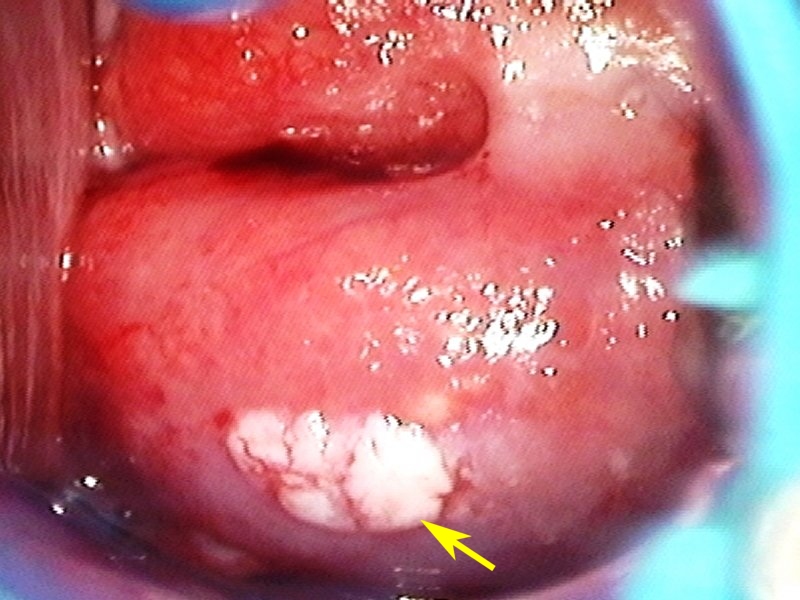
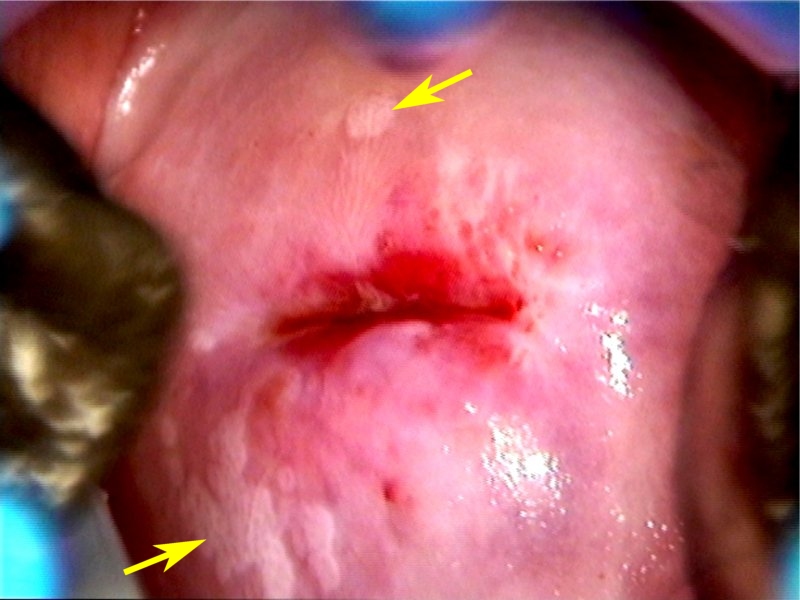
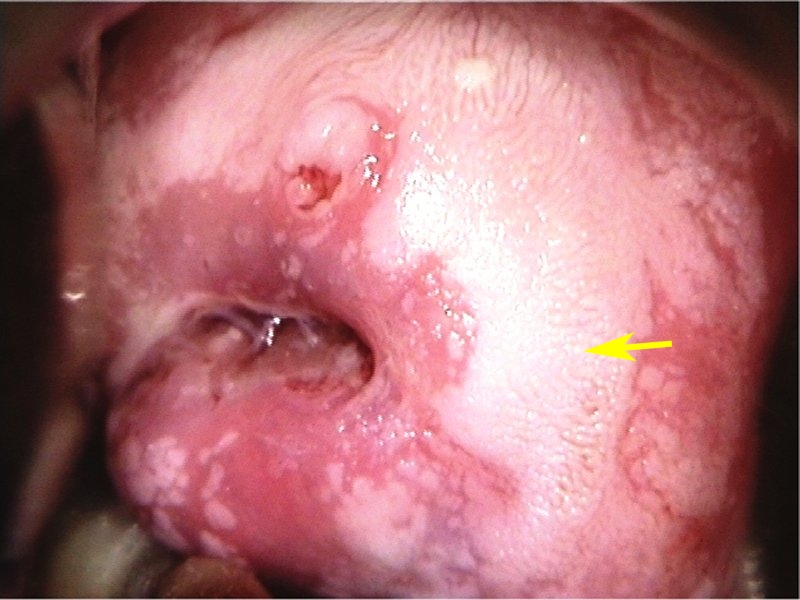
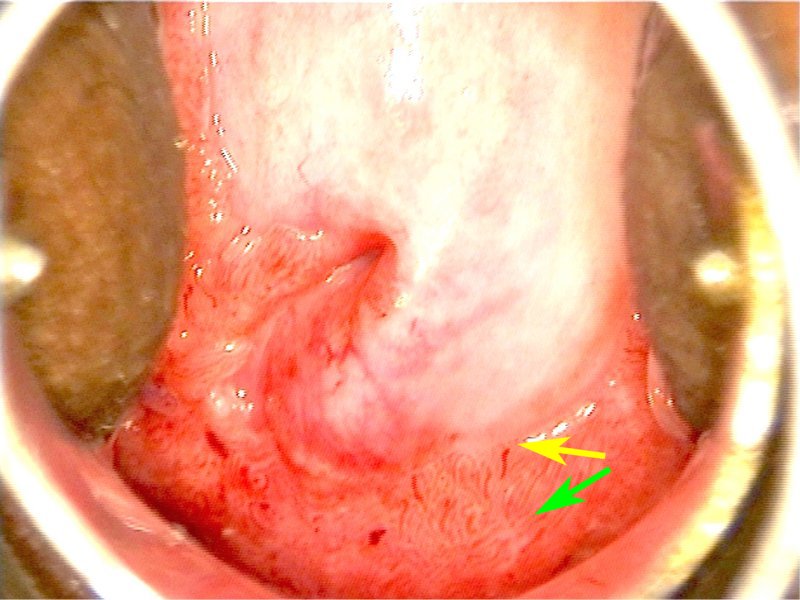
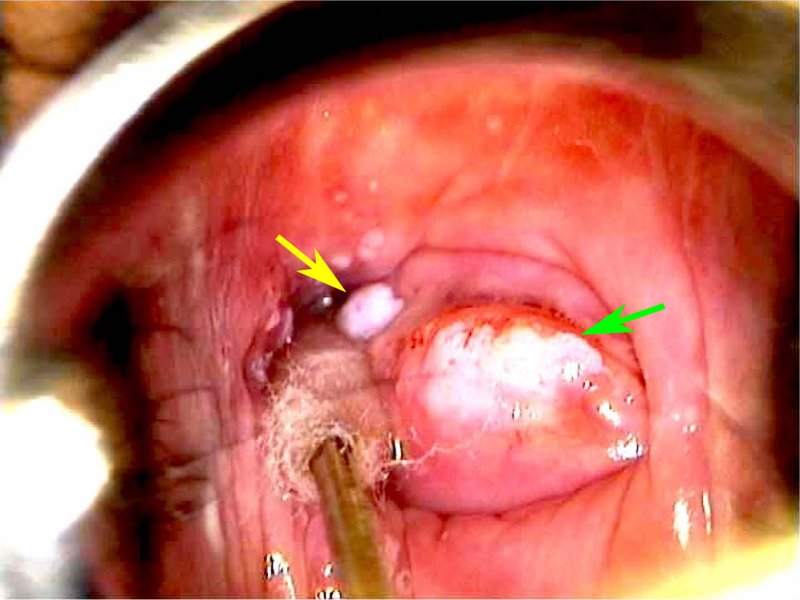
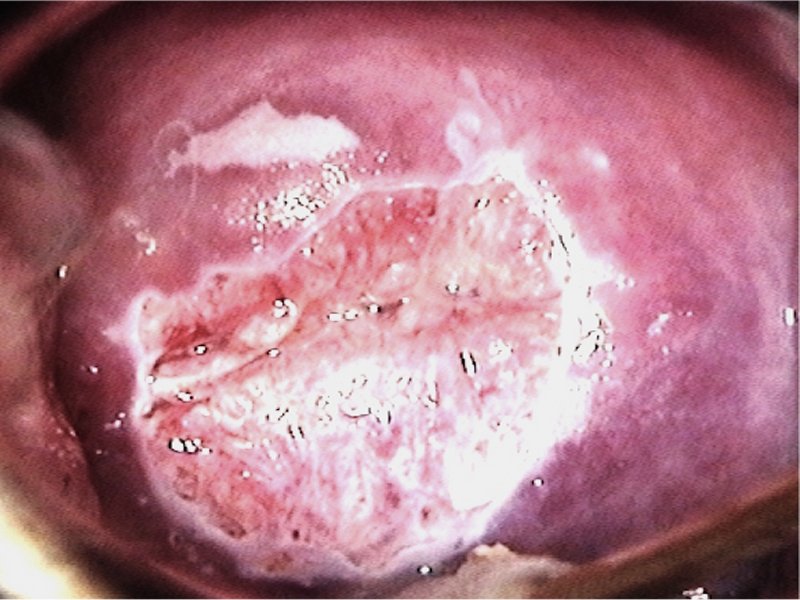
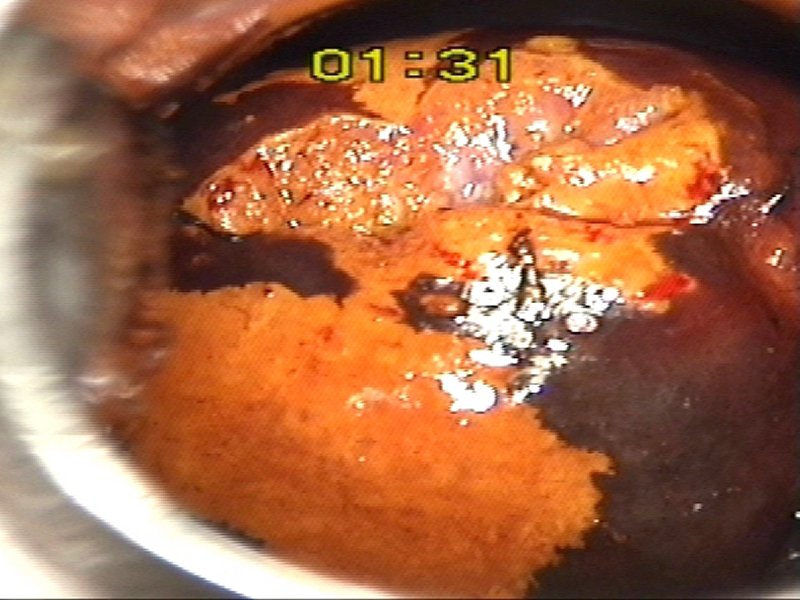
Genital condylomata (warts) are caused by infection with low-risk (non-oncogenic) types of human papillomavirus (HPV). Condylomata can be detected on the external genitalia, vagina, or cervix and are frequently multiple.
Clinically detectable cervical condyloma may appear as single or multiple distinct, lumpy, irregular lesions on the cervix. The colour is usually bright white, and the surface is irregular, pitted, or spiky. The location of condylomata can be anywhere on the cervix. Unlike neoplastic lesions, they are not confined to the TZ. When there are multiple lesions, the lesions away from the SCJ are called satellite lesions. Satellite lesions are typically seen in condylomata. Some of the condylomata have finger-like projections on the surface (papilliferous condyloma) with a central capillary loop in each of the projections. Such a condyloma near the SCJ can be confused with prominent villi of the columnar epithelium. Condylomata as multiple discrete raised white lesions can be seen in the vagina with or without associated cervical lesions. Vulvar condylomata can be a few discrete papillary lesions or multiple exophytic lesions with spiky or finger-like projections on the surface. The majority of condylomata of the cervix are not visible before application of acetic acid. Acetowhite patches with irregular, geographical margins and multiple satellite lesions, often away from the SCJ, are characteristic of these subclinical papillomavirus infections (SPI). The lesions may be milky or thin acetowhite and may have fine mosaics on the surface. Cervical condylomata do not take up iodine after application of Lugols iodine. |


25 avenue Tony Garnier CS 90627 69366, LYON CEDEX 07 France - Tel: +33 (0)4 72 73 84 85
© IARC 2026 - Terms of use - Privacy Policy.
© IARC 2026 - Terms of use - Privacy Policy.