



Home / Reseach Projects / Cervical cancer prevention and early detection
Research projects
Cervical cancer prevention and early detection
CARE4Afrique: Implementation of a pilot cervical cancer screening programme based on a single-visit approach and improving capacity for breast cancer early diagnosis in Benin, Cameroon, Côte dIvoire and Senegal
| Study sites: | Benin, Cameroon, Côte dIvoire and Senegal |
| Principal investigator (PI) from IARC: | P. Basu |
| PIs from collaborating institutions: |
|
| Map: |  |
| Start date: | 2017 |
| Closure date: | Ongoing |
| Objectives: | The third edition of the World Banks publication Disease Control Priorities recommends opportunistic screening using visual inspection with acetic acid (VIA) and treatment of precancerous lesions (the screen-and-treat approach) as part of an essential package of health interventions in low-income countries. But very few countries in sub-Saharan Africa have taken steps to introduce such screen-and-treat programmes. The experience gained from properly implemented pilot projects in these countries will inform pragmatic decision-making by policy-makers in scaling up the programmes. The Disease Control Priorities project also identified early diagnosis of women with breast symptoms linked with access to good-quality treatment as the most practical strategy to tackle the growing burden of breast cancer in countries with limited-resource settings.
The primary objectives of the CARE4Afrique study are to implement and evaluate pilot projects using the VIA screen-and-treat approach, and to increase breast cancer early diagnosis capacity in Benin, Cameroon, Côte dIvoire and Senegal. The study will also evaluate some novel approaches, such as the use of thermocoagulation for the treatment of eligible VIA-positive women. |
| Methodology: | 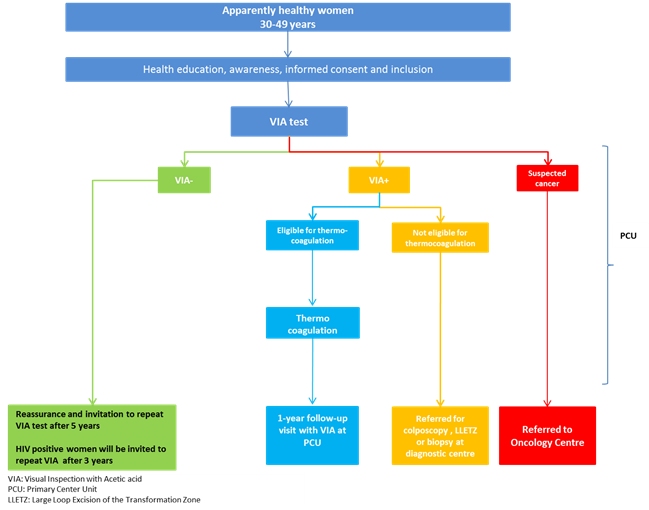 In consultation with the respective Ministries of Health, the study investigators are in the process of selecting two to three primary health centres/district hospitals in each participating country, where trained nurses will provide VIA screen-and-treat services to women aged 3049 years. The investigators will also identify a diagnostic facility in each country where screen-positive women not eligible for thermocoagulation will be referred for colposcopy and treatment. Women with suspected invasive cancers will be referred directly to an oncology centre. Screen-negative women will be advised to undergo repeat VIA after 5 years, unless they are known to be HIV-positive, in which case they will be advised to undergo screening every 3 years. All treated women will be advised to receive follow-up after 1 year. Two master trainers from each country will be trained in a week-long course on cervical cancer prevention, early detection, and management. The master trainers will then train the nurses, general practitioners, and gynaecologists in their respective countries. Programme monitoring will be carried out on a regular basis to assess the following indicators:
|
| Funding: | Lalla Salma Foundation for Cancer Prevention and Treatment | Media: |