



Home / Training / Manuals / Colposcopy and treatment of cervical intraepithelial neoplasia: a beginners manual / Chapter 11: Management that provides continuity of care for women
 figure 11.1: Flow chart of managem...
figure 11.1: Flow chart of managem...
 table 11.1: Treatment for reproduc...
table 11.1: Treatment for reproduc...
 table 11.2: Indications for cold-k...
table 11.2: Indications for cold-k...
Colposcopy and treatment of cervical intraepithelial neoplasia: a beginners manual, Edited by J.W. Sellors and R. Sankaranarayanan
Chapter 11: Management that provides continuity of care for women
Filter by language: English / Français / Español / Portugues / 中文- If women are diagnosed with reproductive tract infection, prompt treatment should be instituted according to the WHO guidelines.
- Though it may be preferred to have the diagnosis of CIN firmly established before treatment is offered, in many low-resource settings, treatment may be offered at the first colposcopy visit, based on colposcopic findings, to maximize treatment coverage.
- The clinical management of women with CIN 1 lesions may take one of the following courses: (i) immediate treatment or (ii) follow the woman and then treat if the lesion is persistent or progressive after 18 to 24 months.
- All women with CIN 2 and CIN 3 lesions should be treated with cryotherapy or LEEP.
- Women diagnosed with invasive cancer should be promptly referred for treatment.
- Women diagnosed with high-grade CIN during pregnancy can be reviewed at about 28 weeks gestation. If the disease is stable, the woman may be reviewed at 2-3 months post-partum for definitive diagnosis by biopsy and appropriate management of lesions.
- Women treated for CIN may be reviewed at 9-12 months after treatment.
Planning a womans medical management after her initial colposcopic assessment is primarily the duty of the colposcopist. It is appropriate to involve the woman, as a partner, in the decision-making process. Management usually depends on the final assessment after the colposcopic findings have been integrated with the pathology reports. Management plans also depend on whether or not the woman is pregnant. The management plan should be explicitly detailed in the medical record and communicated clearly to the patient at the earliest opportunity. Ideally, pathology reports (biopsy, endocervical curettage (ECC), loop electrosurgical excision procedure (LEEP) specimen, cytology) should be available to the colposcopist within three weeks of carrying out the colposcopy. Cryotherapy or LEEP are the two forms of therapy discussed in this manual (see Chapters 12 and 13), but it must be emphasized each has specific indications for their use and should be used only when women fulfil all of the eligibility criteria for the specific therapy. A general plan of management that may be adapted in low-resource settings is shown in Figure 11.1
It is generally preferable to have the diagnosis of cervical intraepithelial neoplasia (CIN) firmly established before a decision on management is taken and any treatment offered. However, there may be exceptions to this rule. For example, in many settings, particularly developing countries, women may be offered treatment at their first colposcopy visit, based on colposcopic assessment to maximize treatment coverage (otherwise patients lost to follow-up would not receive treatment for lesions). If the decision is to treat with cryotherapy, a biopsy (or biopsies) may be directed before cryotherapy, as this type of treatment does not produce a tissue specimen for histological examination. A tissue sample taken before instituting ablative therapy will help to confirm the histological nature of the lesion treated a posteriori. Expert colposcopists also may use this approach to maximize treatment coverage and to minimize the number of clinic visits in some settings. However, this approach may result in a significant degree of overtreatment. Even though it is assumed that treatment methods such cryotherapy and LEEP are safe, and are unlikely to be associated with long-term sequelae and complications, the long-term implications of such overtreatment remains yet to be firmly established. On the other hand, it is likely that overtreatment may, to a certain extent, protect against future development of CIN, in view of the ablation of the transformation zone where the vast majority of CIN lesions occur.
){kind=link}
It is generally preferable to have the diagnosis of cervical intraepithelial neoplasia (CIN) firmly established before a decision on management is taken and any treatment offered. However, there may be exceptions to this rule. For example, in many settings, particularly developing countries, women may be offered treatment at their first colposcopy visit, based on colposcopic assessment to maximize treatment coverage (otherwise patients lost to follow-up would not receive treatment for lesions). If the decision is to treat with cryotherapy, a biopsy (or biopsies) may be directed before cryotherapy, as this type of treatment does not produce a tissue specimen for histological examination. A tissue sample taken before instituting ablative therapy will help to confirm the histological nature of the lesion treated a posteriori. Expert colposcopists also may use this approach to maximize treatment coverage and to minimize the number of clinic visits in some settings. However, this approach may result in a significant degree of overtreatment. Even though it is assumed that treatment methods such cryotherapy and LEEP are safe, and are unlikely to be associated with long-term sequelae and complications, the long-term implications of such overtreatment remains yet to be firmly established. On the other hand, it is likely that overtreatment may, to a certain extent, protect against future development of CIN, in view of the ablation of the transformation zone where the vast majority of CIN lesions occur.
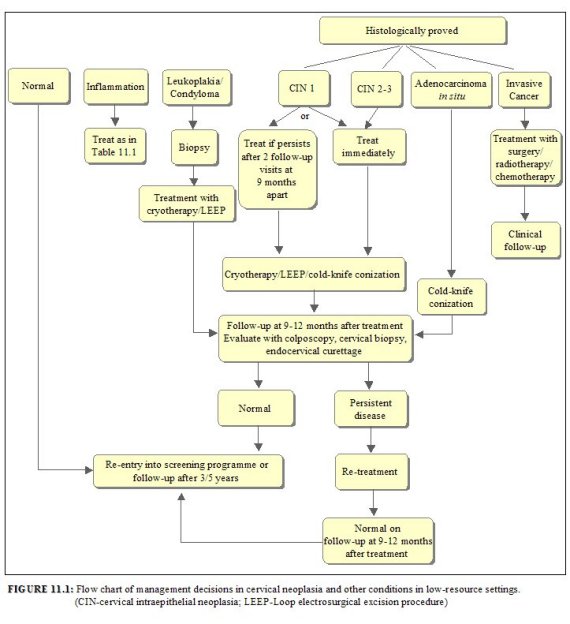 figure 11.1: Flow chart of managem...
figure 11.1: Flow chart of managem...Outcomes after colposcopic assessment
Normal colposcopy outcome
In most women with a normal cervix, assessment using the colposcope results in a satisfactory evaluation of the cervix. If the squamocolumnar junction is visible and there is no colposcopic evidence of CIN or invasive cancer, the woman should be discharged and may resume participation in the screening programme, if one is on-going in the region (which is not the case in many developing countries!). Otherwise, she may be advised to undergo a repeat screening examination after three to five years.
Reproductive tract infection
If a woman is diagnosed with reproductive tract infection, prompt treatment should be instituted following the WHO guidelines ( WHO, 2001). The treatment policies for pregnant and non-pregnant women, diagnosed with reproductive tract infection, are outlined in Table 11.1. Use of oral metronidazole is contraindicated during the first trimester of pregnancy, but can be safely used in the second and third trimesters. Patients taking oral metronidazole should be cautioned not to consume alcohol while they are taking the drug or up to 24 hours after taking the last dose. Patients with advanced syphilis may require prolonged treatment with antibiotics. There is no known cure for genital herpes infections, but the course of symptoms can be modified if systemic therapy with acyclovir or its analogues is initiated.
){kind=link}
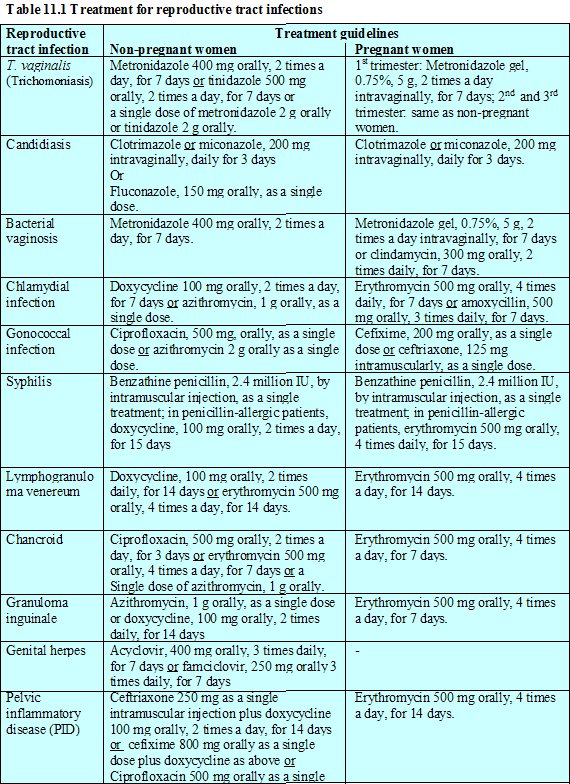 table 11.1: Treatment for reproduc...
table 11.1: Treatment for reproduc...Leukoplakia (hyperkeratosis)
Leukoplakia should be biopsied and submitted for histopathological examination, to rule out underlying cervical neoplasia.
Condyloma
Condylomata should be biopsied and localized ectocervical exophytic lesions may be treated with ablative treatment by cryotherapy or electrofulguration or with excisional treatment such as LEEP.
CIN 1
If the final diagnosis in a woman is CIN 1, the clinical management may take one of the following courses: either to (a) to immediately treat the lesion or (b) follow the woman cytologically or colposcopically and then treat if the lesion is persistent or progressive after 18 to 24 months, and, if regression occurs, discharge her from the colposcopy clinic. In the context of developing countries, a decision may be made to treat the woman, as many fail return for a follow-up visit. If the decision is made to treat the woman with cryotherapy or LEEP, at least one follow-up visit should be scheduled at 9 to 12 months from the date of treatment (see Chapters 12 and 13). After cryotherapy and LEEP, healing of the cervix is grossly apparent by three to four weeks; cytological and colposcopic appearances will continue to reflect healing or regenerative effects for approximately three months. If the follow-up visit reveals no evidence of persistent disease, the woman can be discharged from the colposcopy clinic and advised to participate in the screening programme, if one is on-going in the region. Otherwise, she may be advised to undergo a repeat screening examination after three to five years. If persistent disease is found during the follow-up visit, appropriate investigations and appropriate treatment with cryotherapy, LEEP or cold-knife conization should be carried out.
CIN 2-3
All women with high-grade lesions (CIN 2 or CIN 3) should be treated with cryotherapy or LEEP. They should strictly adhere to management protocols and be scheduled for a follow-up visit at 9 to 12 months after treatment (see Chapters 12 and 13). The woman can be discharged from the colposcopy clinic if the follow-up visit reveals no colposcopic or cytological evidence of persistent disease and she may be advised to resume participation in a screening programme, if one is on-going in the region, or may be followed up after three to five years. If persistent disease is found, the woman should receive appropriate treatment.
If a woman is treated with LEEP for any grade of CIN and the pathology report of a LEEP specimen indicates the possibility of an inadequate excision involving ectocervical or endocervical margins, she should be carefully evaluated in three follow-up visits with cytology, if available, and colposcopy, with special attention to the endocervical canal, at 3, 9 and 15 months. The problem of involved margins needs careful management. If persistent disease is found in any of these follow-up visits, the patient should be treated appropriately and followed up. If there is cytological, ECC or colposcopic evidence of a persistent lesion, and the limits can be seen and are within the range of a LEEP cone, then LEEP may be carried out. Otherwise, a cold-knife conization should be performed to ensure complete removal of the lesion. If the womans results are normal in all three follow-up visits, she may re-enter a screening programme, or be followed up once in three or five years.
If a woman is treated with LEEP for any grade of CIN and the pathology report of a LEEP specimen indicates the possibility of an inadequate excision involving ectocervical or endocervical margins, she should be carefully evaluated in three follow-up visits with cytology, if available, and colposcopy, with special attention to the endocervical canal, at 3, 9 and 15 months. The problem of involved margins needs careful management. If persistent disease is found in any of these follow-up visits, the patient should be treated appropriately and followed up. If there is cytological, ECC or colposcopic evidence of a persistent lesion, and the limits can be seen and are within the range of a LEEP cone, then LEEP may be carried out. Otherwise, a cold-knife conization should be performed to ensure complete removal of the lesion. If the womans results are normal in all three follow-up visits, she may re-enter a screening programme, or be followed up once in three or five years.
Invasive cancer
A diagnosis of invasive squamous cell carcinoma or adenocarcinoma requires prompt referral for definitive treatment with surgery and/or radiotherapy, with or without chemotherapy.
Women requiring further diagnostic investigations
Some cases assessed by colposcopy require more extensive diagnostic investigations before treatment. A mainstay in such investigation of women is cold-knife conization procedure. The indications for diagnostic cone biopsy are shown in Table 11.2. If the CIN lesion extends deep into the endocervical canal (i.e., more than 1.5 cm) or its upper limit is not visible, cold-knife conization is indicated. Women with any cytological report of an abnormality suggesting the possibility of glandular dysplasia should have ECC performed in addition to colposcopic assessment. If ECC does not show evidence of a glandular lesion (but cytology does), cold-knife conization may be indicated. Women with cytology suggestive of adenocarcinoma or with histological evidence of glandular dysplasia or adenocarcinoma should have cold-knife conization to thoroughly evaluate the extent and severity of disease. If adenocarcinoma is found, it should be definitively treated as soon as possible.
){kind=link}
 table 11.2: Indications for cold-k...
table 11.2: Indications for cold-k...Pregnant women
Pregnancy may be a womans first opportunity to be screened for cervical cancer as part of routine prenatal care. In this case, she may often be referred for colposcopy following an abnormal cytology smear result before to the midpoint of the pregnancy. The usual scenarios and recommendations as to how each should be managed are discussed below.
Colposcopists should note that lesions seen in the cervix of a pregnant woman may become smaller post-partum due to shrinkage of the cervix. Lesions will tend to migrate post-partum towards the os due to inversion (the opposite of eversion) of the cervical epithelium. Therefore, a lesion followed into the post-partum period may appear smaller and may be located more into the canal than on the ectocervix.
During pregnancy, it is considered adequate management to base a working diagnosis on a colposcopic assessment of CIN without biopsy confirmation. If there is any slight doubt that the disease may be invasive cancer, a biopsy should be obtained. Since referral and colposcopic diagnosis usually occur near the midpoint of pregnancy, the woman in whom a high-grade CIN is suspected may be reviewed at about 28 weeks gestation. Cytological and colposcopic examinations should be performed at both visits. If the cytological or colposcopic diagnosis changes to a more severe degree of abnormality at any of the follow-up visits during pregnancy, a directed punch biopsy should be obtained. If the disease is stable, the woman can be seen at two to three months post-partum for definitive diagnosis by biopsy and appropriate management of any lesion(s). The management plans for women at post-partum follow-up visits depend on the final diagnosis, and correspond to those described for nonpregnant women.
Vaginal delivery can be allowed if microinvasion or CIN is confirmed and definitive post-partum reassessment and treatment are planned. These women should be seen for definitive reassessment at 8 to 12 weeks post-partum. The cervix should be completely involuted and/or healed before re-colposcopy.
Colposcopists should note that lesions seen in the cervix of a pregnant woman may become smaller post-partum due to shrinkage of the cervix. Lesions will tend to migrate post-partum towards the os due to inversion (the opposite of eversion) of the cervical epithelium. Therefore, a lesion followed into the post-partum period may appear smaller and may be located more into the canal than on the ectocervix.
During pregnancy, it is considered adequate management to base a working diagnosis on a colposcopic assessment of CIN without biopsy confirmation. If there is any slight doubt that the disease may be invasive cancer, a biopsy should be obtained. Since referral and colposcopic diagnosis usually occur near the midpoint of pregnancy, the woman in whom a high-grade CIN is suspected may be reviewed at about 28 weeks gestation. Cytological and colposcopic examinations should be performed at both visits. If the cytological or colposcopic diagnosis changes to a more severe degree of abnormality at any of the follow-up visits during pregnancy, a directed punch biopsy should be obtained. If the disease is stable, the woman can be seen at two to three months post-partum for definitive diagnosis by biopsy and appropriate management of any lesion(s). The management plans for women at post-partum follow-up visits depend on the final diagnosis, and correspond to those described for nonpregnant women.
Vaginal delivery can be allowed if microinvasion or CIN is confirmed and definitive post-partum reassessment and treatment are planned. These women should be seen for definitive reassessment at 8 to 12 weeks post-partum. The cervix should be completely involuted and/or healed before re-colposcopy.