Using Human Papillomavirus (HPV) detection tests for cervical cancer screening and managing HPV-positive women a practical guide / Activity 3
Neoplastic changes of the cervical epithelium Cervical intraepithelial neoplasia (CIN) | Click on the pictures to magnify and display the legends |
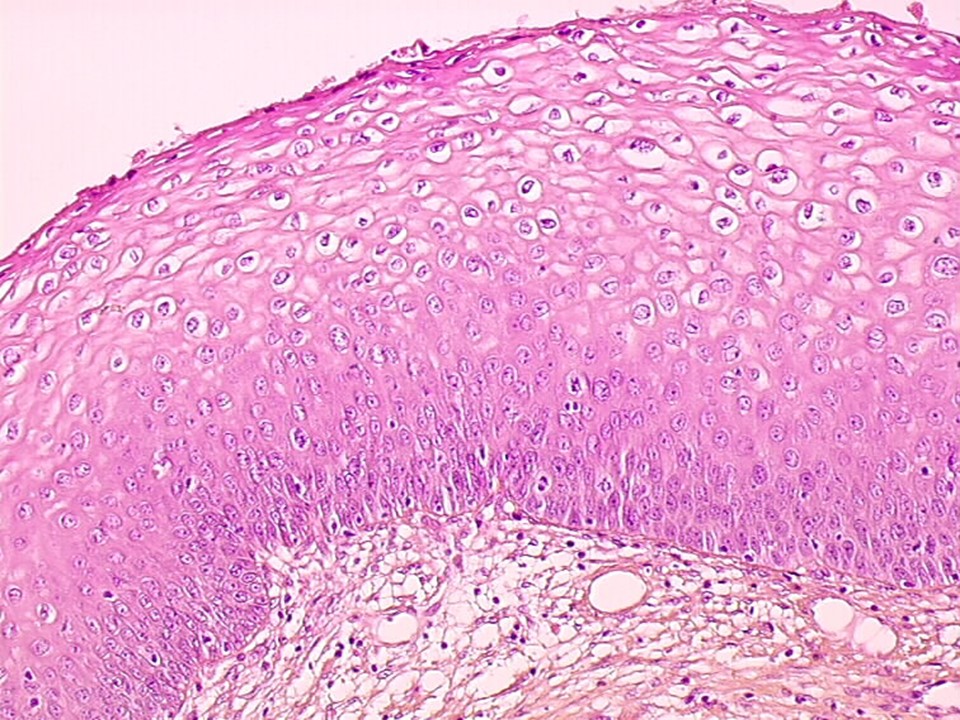
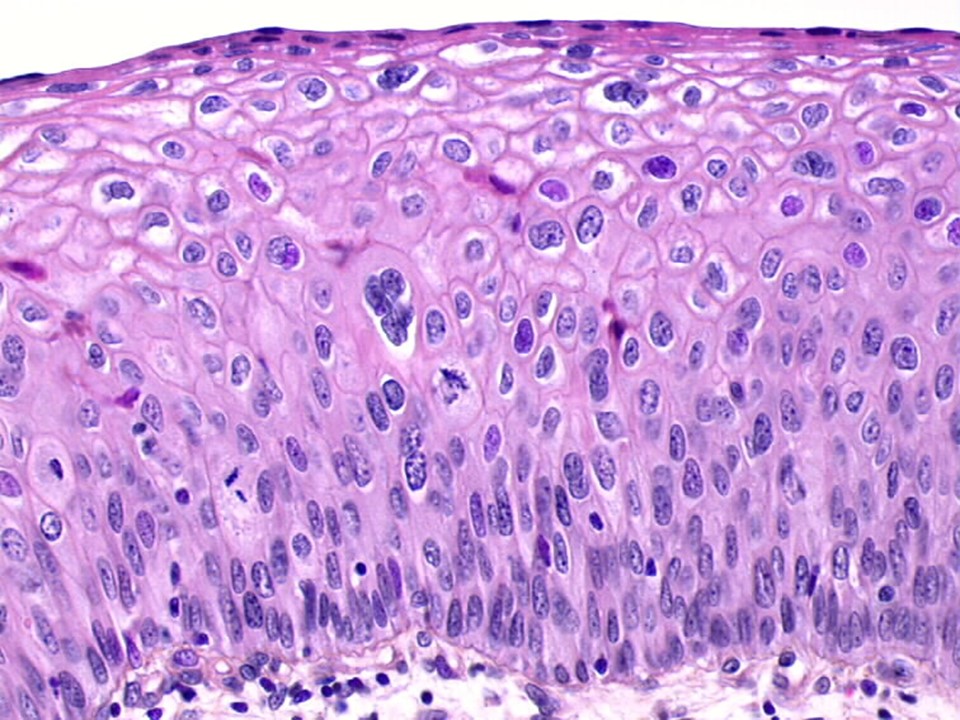
Cervical intraepithelial neoplasia (CIN) is a precancerous condition because the abnormalities are restricted to the thickness of the squamous epithelium. The neoplastic cells do not breach the basement membrane to invade deeper into the stroma or beyond. Depending on the severity of the abnormality and the extent of involvement of the thickness of the squamous epithelium, CIN lesions are graded as CIN1, CIN2, and CIN3.
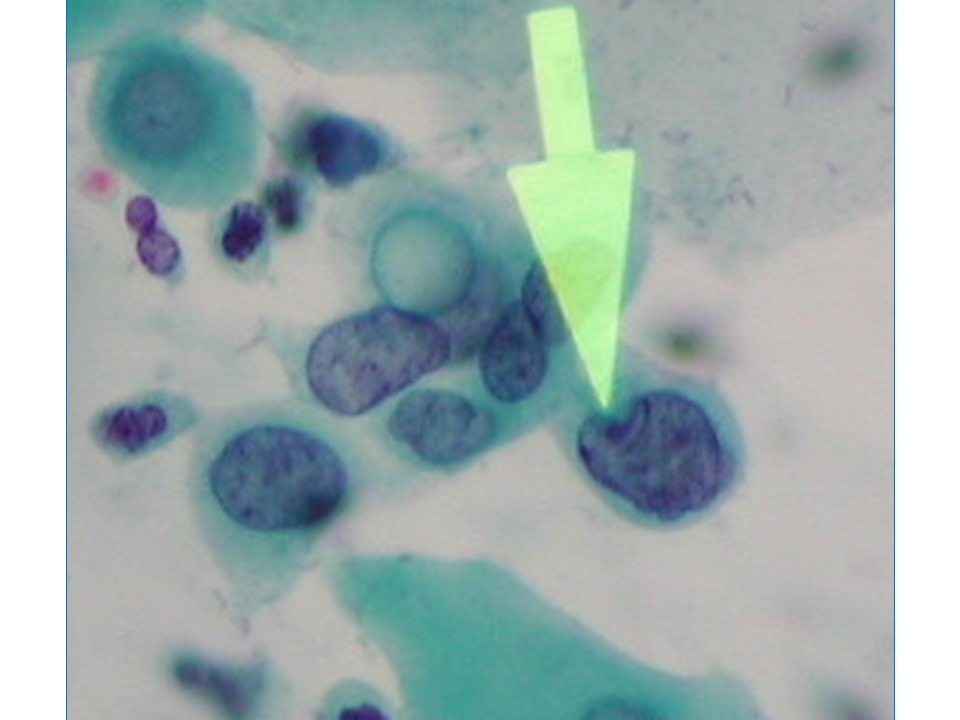
The neoplastic cells present in CIN have a higher nuclearcytoplasmic ratio compared with normal cells, an irregular nuclear membrane, dense chromatin in the nucleus, and mitotic figures. These features increase in prominence with higher grade of neoplasia. In addition, the normal systematic arrangement of the different layers of the epithelium is lost (this is called a loss of polarity) as the cells become cancerous. CIN1 is the earliest form of CIN, in which the neoplastic cells are limited to the lower third of the thickness of the cervical epithelium. Most of these lesions are caused by a transient HPV infection and disappear with the clearance of the HPV infection. The abnormal cells have the classic features of HPV infection. These cells (also known as koilocytes) have an empty and irregular zone (a halo) around the nucleus, and the nucleus is often larger in size, with irregular borders. In CIN2 and CIN3, the cervical epithelial abnormalities extend to the middle third and the upper third of the thickness of the cervical epithelium, respectively, and the cellular abnormalities become progressively more severe. The rapidly dividing abnormal cells cannot accumulate glycogen, and the cytoplasm remains intact. CIN1 lesions rarely progress to invasive cancer, but about 3050% of CIN3 lesions will progress to invasive cancer if left untreated. The potential of CIN2 to progress further is somewhere between that of CIN1 and that of CIN3. CIN1 lesions are also known as low-grade squamous intraepithelial lesions (LSIL), because of the low potential for progression. CIN2 and CIN3 lesions are grouped together as high-grade squamous intraepithelial lesions (HSIL).
The next section provides more information about glandular precancers: adenocarcinoma in situ. |